

Brief FASD prevention intervention: physicians' skills demonstrated in a clinical trial in Russia
- PMID: 23294846
- PMCID: PMC3685594
- DOI: 10.1186/1940-0640-8-1
Brief FASD prevention intervention: physicians' skills demonstrated in a clinical trial in Russia
Abstract
Background: Alcohol consumption during pregnancy can result in a range of adverse pregnancy outcomes including Fetal Alcohol Spectrum Disorders (FASD). Risky drinking among Russian women constitutes a significant risk for alcohol-exposed pregnancies (AEP). Russian women report that obstetrics and gynecology (OB/GYN) physicians are the most important source of information about alcohol consumption during pregnancy and developing effective prevention interventions by OB/GYNs is indicated. This is the first study focused on implementation of an AEP prevention intervention at women's clinics in Russia.
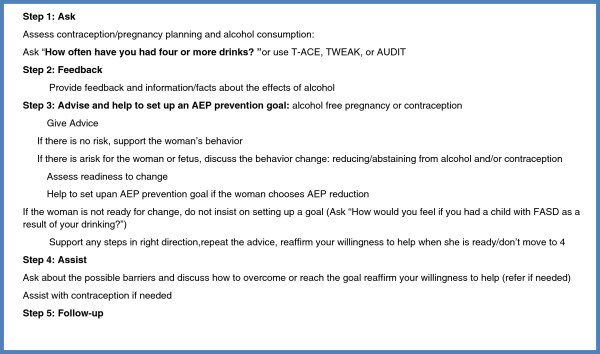
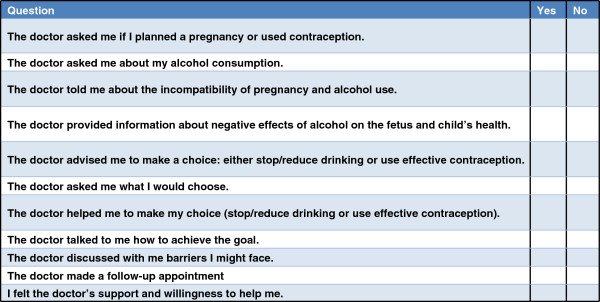
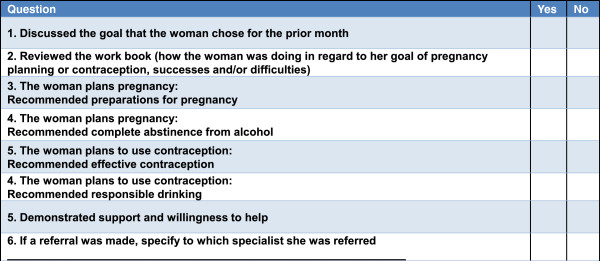
Method: The paper describes the intervention protocol and addresses questions about the feasibility of a brief FASD prevention intervention delivered by OB/GYNs at women's clinics in Russia. Brief physician intervention guidelines and two evidence-based FASD prevention interventions were utilized to design a brief dual-focused physician intervention (DFBPI) appropriate to Russian OB/GYN care. The questions answered were whether trained OB/GYN physicians could deliver DFBPI during women's routine clinic visits, whether they maintained skills over time in clinical settings, and which specific intervention components were better maintained. Data were collected as part of a larger study aimed at evaluating effectiveness of DFBPI in reducing AEP risk in non-pregnant women. Methods of monitoring the intervention delivery included fidelity check lists (FCL) with the key components of the intervention completed by physicians and patients and live and audio taped observations of intervention sessions. Physicians (N = 23) and women (N = 372) independently completed FCL, and 78 audiotapes were coded.
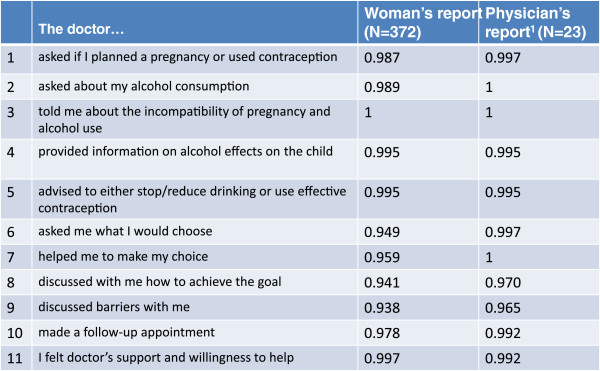
Results: The differences between women's and physicians' reports on individual items were not significant. Although the majority of physician and patient reports were consistent (N = 305), a discrepancy existed between the reports in 57 cases. Women reported more intervention components missing compared to physicians (p < 0.001). Discussing barriers was the most difficult component for physicians to implement, and OB/GYN demonstrated difficulties in discussing contraception methods.
Conclusions: The results supported the feasibility of the DFBPI in Russia. OB/GYN physicians trained in the DFBPI, monitored, and supported were able to implement and maintain skills during the study. In addition to the alcohol focus, DFBPI training needs to have a sufficient component to improve physicians' skills in discussing contraception use.
Figures
References
-
- American Academy of Pediatrics Committee on Substance Abuse and Committee on Children With Disabilities. Fetal alcohol syndrome and alcohol-related neurodevelopmental disorders. Pediatrics. 2000;106:358–361. - PubMed
-
- Bertrand J, Floyd RL, Weber MK, O’Connor M, Riley EP, Johnson KA, Cohen DE. National Task Force on FAS/FAE. Fetal Alcohol Syndrome: Guidelines for Referral and Diagnosis. Atlanta: Centers for Disease Control and Prevention; 2004.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
