

Early sepsis does not increase the risk of late sepsis in very low birth weight neonates
- PMID: 23295144
- PMCID: PMC3622770
- DOI: 10.1016/j.jpeds.2012.11.027
Early sepsis does not increase the risk of late sepsis in very low birth weight neonates
Abstract
Objective: To examine whether preterm very low birth weight (VLBW) infants have an increased risk of late-onset sepsis (LOS) following early-onset sepsis (EOS).
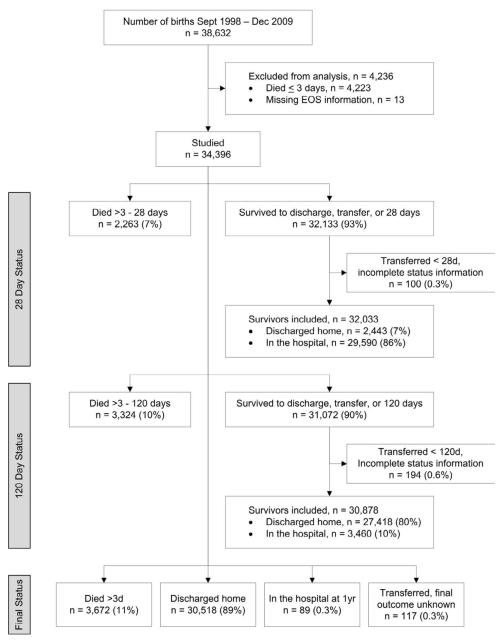
Study design: Retrospective analysis of VLBW infants (401-1500 g) born September 1998 through December 2009 who survived >72 hours and were cared for within the National Institute of Child Health and Human Development Neonatal Research Network. Sepsis was defined by growth of bacteria or fungi in a blood culture obtained ≤ 72 hours of birth (EOS) or >72 hours (LOS) and antimicrobial therapy for ≥ 5 days or death <5 days while receiving therapy. Regression models were used to assess risk of death or LOS by 120 days and LOS by 120 days among survivors to discharge or 120 days, adjusting for gestational age and other covariates.
Results: Of 34,396 infants studied, 504 (1.5%) had EOS. After adjustment, risk of death or LOS by 120 days did not differ overall for infants with EOS compared with those without EOS [risk ratio (RR): 0.99 (0.89-1.09)] but was reduced in infants born at <25 weeks gestation [RR: 0.87 (0.76-0.99), P = .048]. Among survivors, no difference in LOS risk was found overall for infants with versus without EOS [RR: 0.88 (0.75-1.02)], but LOS risk was reduced in infants with birth weight 401-750 g who had EOS [RR: 0.80 (0.64-0.99), P = .047].
Conclusions: Risk of LOS after EOS was not increased in VLBW infants. Surprisingly, risk of LOS following EOS appeared to be reduced in the smallest, most premature infants, underscoring the need for age-specific analyses of immune function.
Copyright © 2013 Mosby, Inc. All rights reserved.
Figures
Similar articles
-
Very low birth weight preterm infants with early onset neonatal sepsis: the predominance of gram-negative infections continues in the National Institute of Child Health and Human Development Neonatal Research Network, 2002-2003.Pediatr Infect Dis J. 2005 Jul;24(7):635-9. doi: 10.1097/01.inf.0000168749.82105.64. Pediatr Infect Dis J. 2005. PMID: 15999007
-
Late-Onset Sepsis in Very Low Birth Weight Premature Infants: A 10-Year Review of a Brazilian Tertiary University Hospital-the Challenge Remains.Am J Perinatol. 2024 May;41(S 01):e1725-e1731. doi: 10.1055/s-0043-1768702. Epub 2023 May 11. Am J Perinatol. 2024. PMID: 37168011
-
Blood Culture Proven Early Onset Sepsis and Late Onset Sepsis in Very-Low-Birth-Weight Infants in Korea.J Korean Med Sci. 2015 Oct;30 Suppl 1(Suppl 1):S67-74. doi: 10.3346/jkms.2015.30.S1.S67. Epub 2015 Oct 27. J Korean Med Sci. 2015. PMID: 26566360 Free PMC article.
-
Association of Histological and Clinical Chorioamnionitis With Neonatal Sepsis Among Preterm Infants: A Systematic Review, Meta-Analysis, and Meta-Regression.Front Immunol. 2020 Jun 5;11:972. doi: 10.3389/fimmu.2020.00972. eCollection 2020. Front Immunol. 2020. PMID: 32582153 Free PMC article.
-
Management of Neonates Born at ≤34 6/7 Weeks' Gestation With Suspected or Proven Early-Onset Bacterial Sepsis.Pediatrics. 2018 Dec;142(6):e20182896. doi: 10.1542/peds.2018-2896. Pediatrics. 2018. PMID: 30455344 Review.
Cited by
-
Innate immune memory: implications for development of pediatric immunomodulatory agents and adjuvanted vaccines.Pediatr Res. 2014 Jan;75(1-2):184-8. doi: 10.1038/pr.2013.214. Epub 2013 Nov 6. Pediatr Res. 2014. PMID: 24352476 Free PMC article. Review.
-
Protective Role of an Initial Low-Dose Septic Challenge against Lethal Sepsis in Neonatal Mice: A Pilot Study.J Clin Med. 2021 Dec 13;10(24):5823. doi: 10.3390/jcm10245823. J Clin Med. 2021. PMID: 34945120 Free PMC article.
-
Impact of Early-Life Exposures to Infections, Antibiotics, and Vaccines on Perinatal and Long-term Health and Disease.Front Immunol. 2017 Jun 23;8:729. doi: 10.3389/fimmu.2017.00729. eCollection 2017. Front Immunol. 2017. PMID: 28690615 Free PMC article. Review.
-
Sepsis-Induced Immunosuppression in Neonates.Front Pediatr. 2018 Nov 29;6:357. doi: 10.3389/fped.2018.00357. eCollection 2018. Front Pediatr. 2018. PMID: 30555806 Free PMC article. Review.
-
Adverse Events After Routine Immunization of Extremely Low-Birth-Weight Infants.JAMA Pediatr. 2015 Aug;169(8):740-5. doi: 10.1001/jamapediatrics.2015.0418. JAMA Pediatr. 2015. PMID: 26030302 Free PMC article.
References
Publication types
MeSH terms
Grants and funding
- U10 HD27851/HD/NICHD NIH HHS/United States
- U10 HD40689/HD/NICHD NIH HHS/United States
- M01 RR44/RR/NCRR NIH HHS/United States
- U10 HD021364/HD/NICHD NIH HHS/United States
- U10 HD40521/HD/NICHD NIH HHS/United States
- M01 RR7122/RR/NCRR NIH HHS/United States
- UL1 TR000454/TR/NCATS NIH HHS/United States
- HHSN275201000003I/HD/NICHD NIH HHS/United States
- 1U10-HD45962-06/HD/NICHD NIH HHS/United States
- U10 HD21385/HD/NICHD NIH HHS/United States
- M01 RR32/RR/NCRR NIH HHS/United States
- 1R01FD003519-01/FD/FDA HHS/United States
- U10 HD40492/HD/NICHD NIH HHS/United States
- U10 HD53119/HD/NICHD NIH HHS/United States
- M01 RR59/RR/NCRR NIH HHS/United States
- M01 RR6022/RR/NCRR NIH HHS/United States
- U10 HD53124/HD/NICHD NIH HHS/United States
- U10 HD21364/HD/NICHD NIH HHS/United States
- U10 HD34216/HD/NICHD NIH HHS/United States
- M01 RR70/RR/NCRR NIH HHS/United States
- U10 HD36790/HD/NICHD NIH HHS/United States
- U10 HD053109/HD/NICHD NIH HHS/United States
- U10 HD27880/HD/NICHD NIH HHS/United States
- HHSN275201000003C/HD/NICHD NIH HHS/United States
- U10 HD27904/HD/NICHD NIH HHS/United States
- M01 RR125/RR/NCRR NIH HHS/United States
- UL1 TR001449/TR/NCATS NIH HHS/United States
- M01 RR633/RR/NCRR NIH HHS/United States
- U10 HD53109/HD/NICHD NIH HHS/United States
- U10 HD40498/HD/NICHD NIH HHS/United States
- 1R01HD057956-02/HD/NICHD NIH HHS/United States
- U10 HD53089/HD/NICHD NIH HHS/United States
- U10 HD27871/HD/NICHD NIH HHS/United States
- M01 RR64/RR/NCRR NIH HHS/United States
- U10 HD27856/HD/NICHD NIH HHS/United States
- U10 HD40461/HD/NICHD NIH HHS/United States
- U10 HD27853/HD/NICHD NIH HHS/United States
- M01 RR39/RR/NCRR NIH HHS/United States
- UL1 TR000041/TR/NCATS NIH HHS/United States
- HHSN267200700051C/HD/NICHD NIH HHS/United States
- M01 RR80/RR/NCRR NIH HHS/United States
- M01 RR16587/RR/NCRR NIH HHS/United States
- U10 HD21397/HD/NICHD NIH HHS/United States
- 1K24HD058735-01/HD/NICHD NIH HHS/United States
- M01 RR54/RR/NCRR NIH HHS/United States
- M01 RR997/RR/NCRR NIH HHS/United States
- U10 HD21373/HD/NICHD NIH HHS/United States
- UG1 HD053109/HD/NICHD NIH HHS/United States
- M01 RR750/RR/NCRR NIH HHS/United States
- UL1 RR24139/RR/NCRR NIH HHS/United States
- U10 HD27881/HD/NICHD NIH HHS/United States
- U10HD21415/HD/NICHD NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
