

Risk of therapy-related secondary leukemia in Hodgkin lymphoma: the Stanford University experience over three generations of clinical trials
- PMID: 23295809
- PMCID: PMC3565182
- DOI: 10.1200/JCO.2012.44.5791
Risk of therapy-related secondary leukemia in Hodgkin lymphoma: the Stanford University experience over three generations of clinical trials
Abstract
Purpose: To assess therapy-related acute myeloid leukemia/myelodysplastic syndrome (t-AML/MDS) risk in patients treated for Hodgkin lymphoma (HL) on successive generations of Stanford clinical trials.
Patients and methods: Patients with HL treated at Stanford with at least 5 years of follow-up after completing therapy were identified from our database. Records were reviewed for outcome and development of t-AML/MDS.
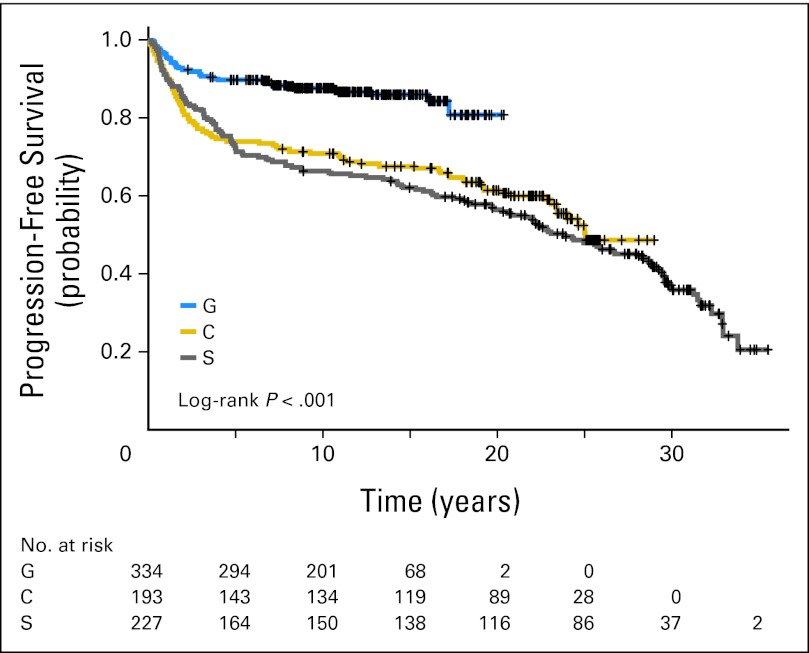
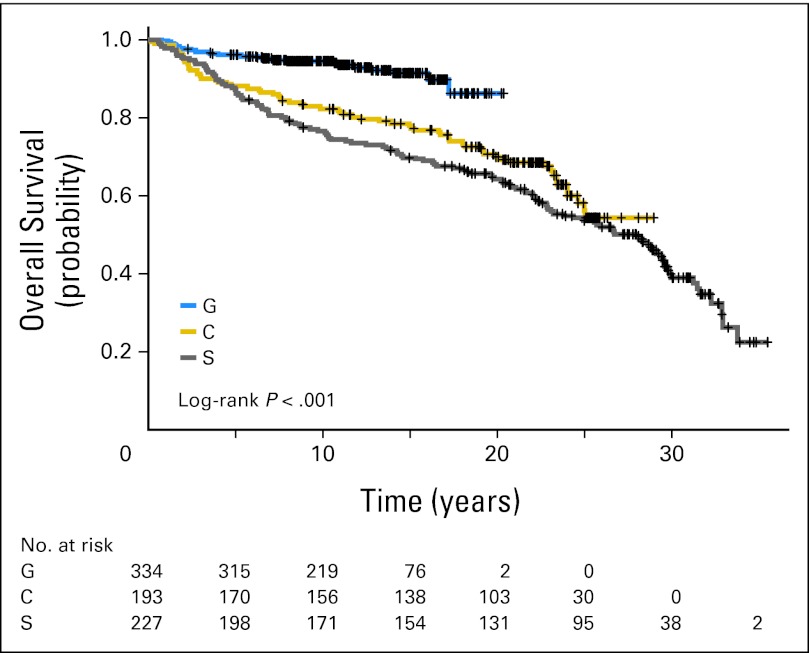
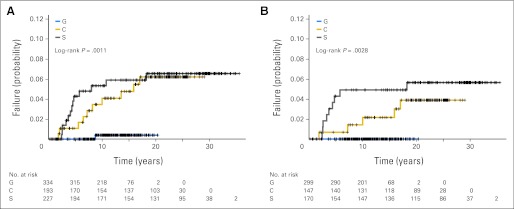
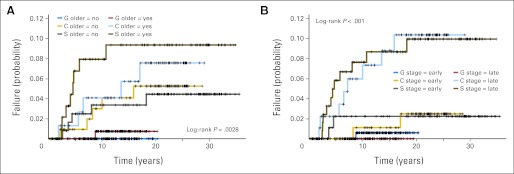
Results: Seven hundred fifty-four patients treated from 1974 to 2003 were identified. Therapy varied across studies. Radiotherapy evolved from extended fields (S and C studies) to involved fields (G studies). Primary chemotherapy was mechlorethamine, vincristine, procarbazine, and prednisone (MOPP) or procarbazine, mechlorethamine, and vinblastine (PAVe) in S studies; MOPP, PAVe, vinblastine, bleomycin, and methotrexate (VBM), or doxorubicin, bleomycin, vinblastine, and dacarbazine (ABVD) in C studies; and VbM (reduced dose of bleomycin compared with VBM) or mechlorethamine, doxorubicin, vinblastine, vincristine, bleomycin, etoposide, and prednisone (Stanford V) in G studies. Cumulative exposure to alkylating agent (AA) was notably lower in the G studies compared with the S and C studies, with a 75% to 83% lower dose of nitrogen mustard in addition to omission of procarbazine and melphalan. Twenty-four (3.2%) of 754 patients developed t-AML/MDS, 15 after primary chemotherapy and nine after salvage chemotherapy for relapsed HL. The incidence of t-AML/MDS was significantly lower in the G studies (0.3%) compared with the S (5.7%) or C (5.2%) studies (P < .001). Additionally, in the G studies, no t-AML/MDS was noted after primary therapy, and the only patient who developed t-AML/MDS did so after second-line therapy.
Conclusion: Our data demonstrate the relationship between the cumulative AA dose and t-AML/MDS. Limiting the dose of AA and decreased need for secondary treatments have significantly reduced the incidence of t-AML/MDS, which was extremely rare in the G studies (Stanford V era).
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
References
-
- Boivin JF, Hutchison GB, Zauber AG, et al. Incidence of second cancers in patients treated for Hodgkin's disease. J Natl Cancer Inst. 1995;87:732–741. - PubMed
-
- van Leeuwen FE, Klokman WJ, Hagenbeek A, et al. Second cancer risk following Hodgkin's disease: A 20-year follow-up study. J Clin Oncol. 1994;12:312–325. - PubMed
-
- Hoppe RT. Hodgkin's disease: Complications of therapy and excess mortality. Ann Oncol. 1997;8(suppl 1):115–118. - PubMed
-
- Kaldor JM, Day NE, Clarke EA, et al. Leukemia following Hodgkin's disease. N Engl J Med. 1990;322:7–13. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
