

The thalamus and multiple sclerosis: modern views on pathologic, imaging, and clinical aspects
- PMID: 23296131
- PMCID: PMC3589190
- DOI: 10.1212/WNL.0b013e31827b910b
The thalamus and multiple sclerosis: modern views on pathologic, imaging, and clinical aspects
Abstract
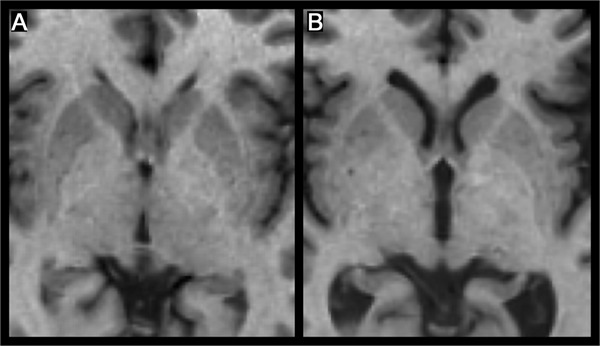
The paired thalamic nuclei are gray matter (GM) structures on both sides of the third ventricle that play major roles in cortical activation, relaying sensory information to the higher cortical centers that influence cognition. Multiple sclerosis (MS) is an immune-mediated disease of the human CNS that affects both the white matter (WM) and GM. A number of clinical observations as well as recent neuropathologic and neuroimaging studies have clearly demonstrated extensive involvement of the thalamus, basal ganglia, and neocortex in patients with MS. Modern MRI techniques permit visualization of GM lesions and measurement of atrophy. These contemporary methods have fundamentally altered our understanding of the pathophysiologic nature of MS. Evidence confirms the contention that GM injury can be detected in the earliest phases of MS, and that iron deposition and atrophy of deep gray nuclei are closely related to the magnitude of inflammation. Extensive involvement of GM, and particularly of the thalamus, is associated with a wide range of clinical manifestations including cognitive decline, motor deficits, fatigue, painful syndromes, and ocular motility disturbances in patients with MS. In this review, we characterize the neuropathologic, neuroimaging, and clinical features of thalamic involvement in MS. Further, we underscore the contention that neuropathologic and neuroimaging correlative investigations of thalamic derangements in MS may elucidate not heretofore considered pathobiological underpinnings germane to understanding the ontogeny, magnitude, and progression of the disease process.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical