

Annual Report to the Nation on the Status of Cancer, 1975-2009, featuring the burden and trends in human papillomavirus(HPV)-associated cancers and HPV vaccination coverage levels
- PMID: 23297039
- PMCID: PMC3565628
- DOI: 10.1093/jnci/djs491
Annual Report to the Nation on the Status of Cancer, 1975-2009, featuring the burden and trends in human papillomavirus(HPV)-associated cancers and HPV vaccination coverage levels
Abstract
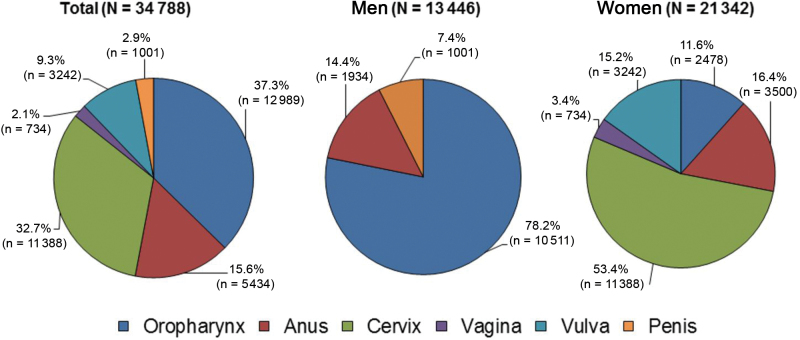
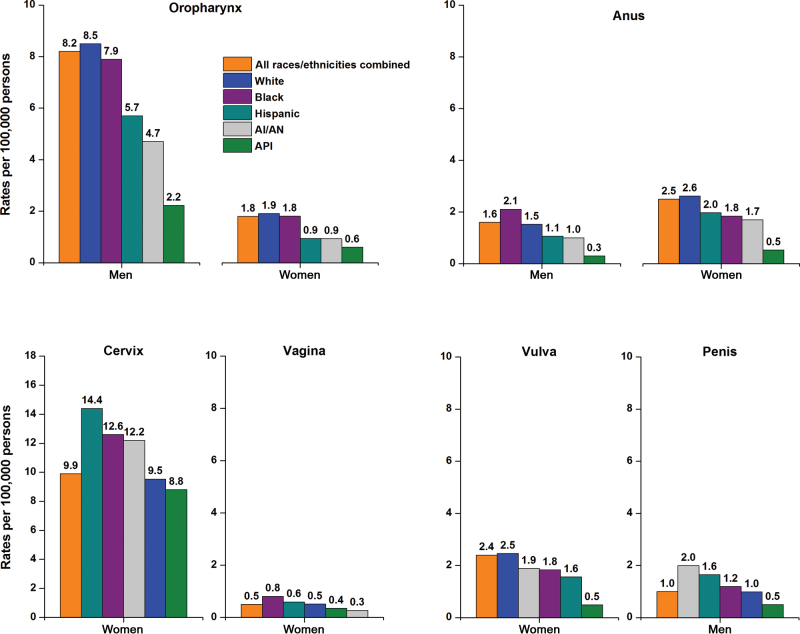
Background: The American Cancer Society (ACS), the Centers for Disease Control and Prevention (CDC), the National Cancer Institute (NCI), and the North American Association of Central Cancer Registries (NAACCR) collaborate annually to provide updates on cancer incidence and death rates and trends in these outcomes for the United States. This year's report includes incidence trends for human papillomavirus (HPV)-associated cancers and HPV vaccination (recommended for adolescents aged 11-12 years).
Methods: Data on cancer incidence were obtained from the CDC, NCI, and NAACCR, and data on mortality were obtained from the CDC. Long- (1975/1992-2009) and short-term (2000-2009) trends in age-standardized incidence and death rates for all cancers combined and for the leading cancers among men and among women were examined by joinpoint analysis. Prevalence of HPV vaccination coverage during 2008 and 2010 and of Papanicolaou (Pap) testing during 2010 were obtained from national surveys.
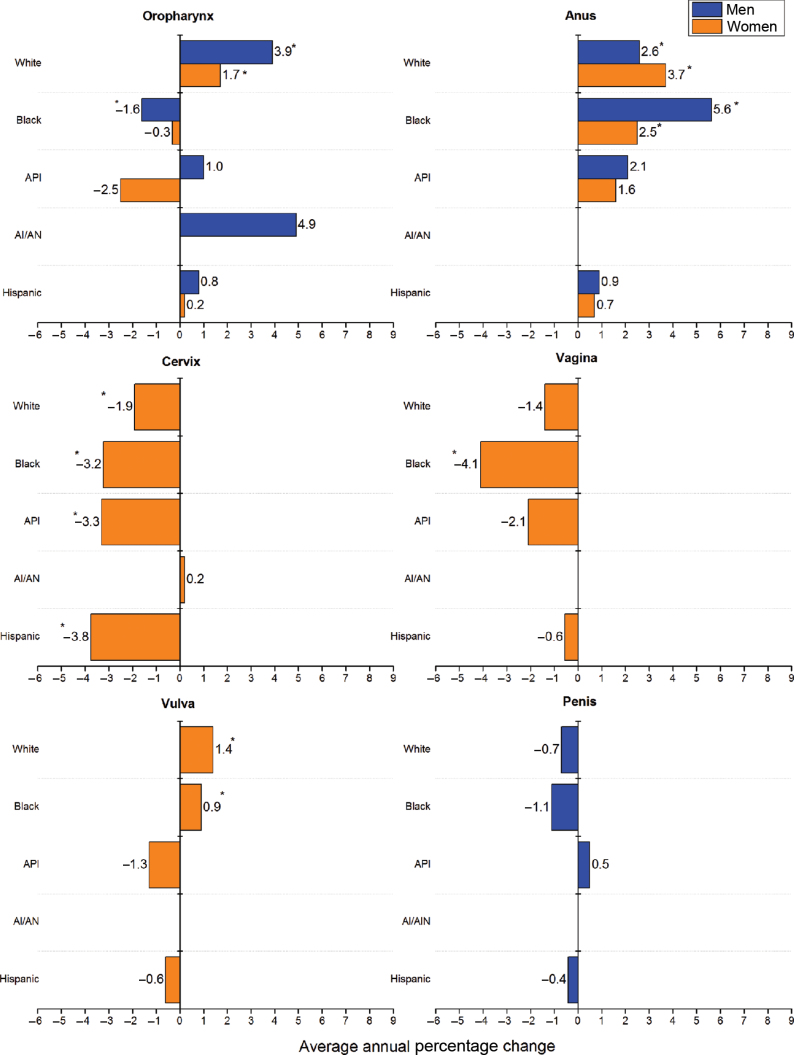
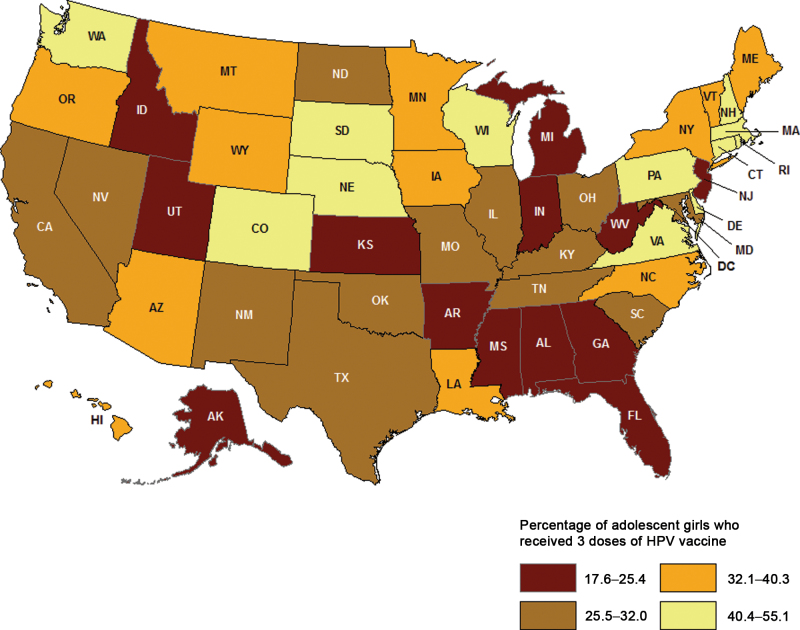
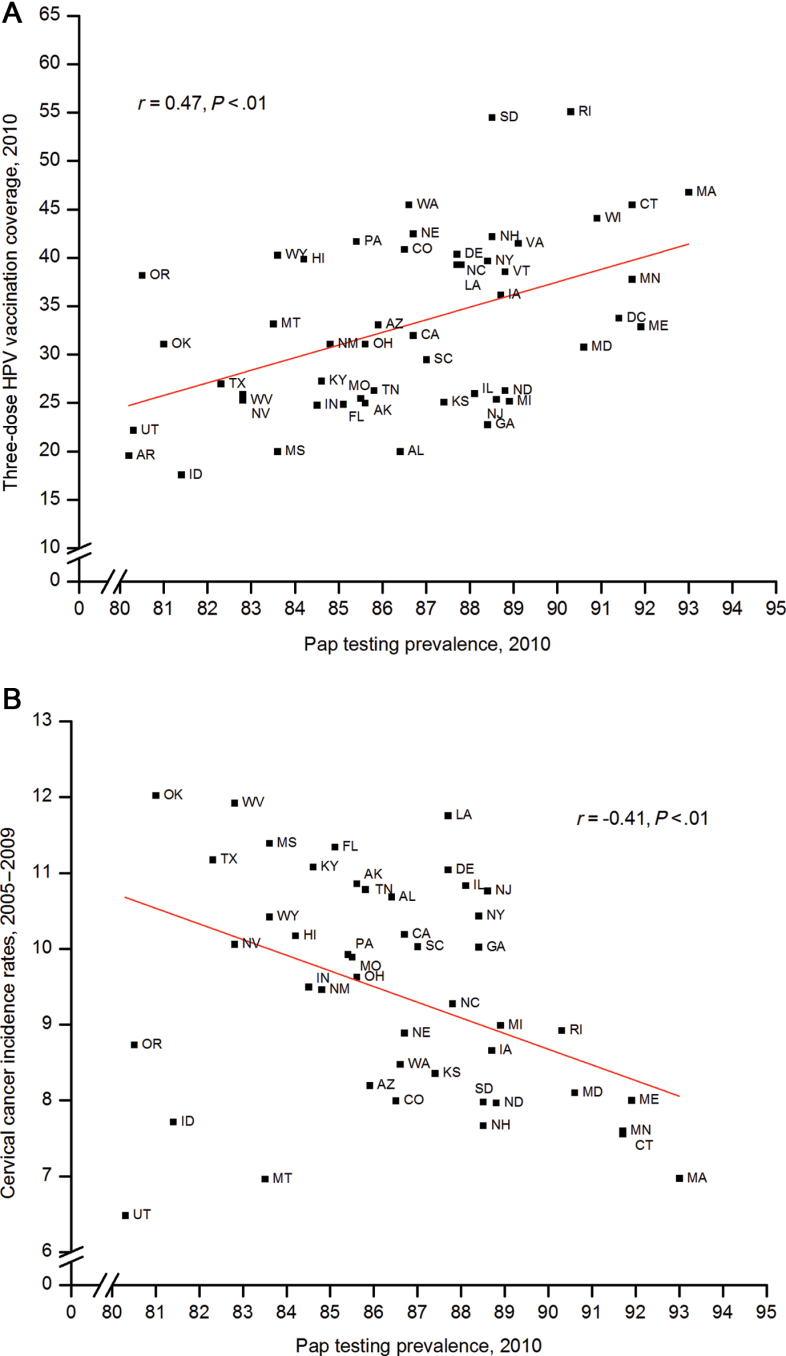
Results: Death rates continued to decline for all cancers combined for men and women of all major racial and ethnic groups and for most major cancer sites; rates for both sexes combined decreased by 1.5% per year from 2000 to 2009. Overall incidence rates decreased in men but stabilized in women. Incidence rates increased for two HPV-associated cancers (oropharynx, anus) and some cancers not associated with HPV (eg, liver, kidney, thyroid). Nationally, 32.0% (95% confidence interval [CI] = 30.3% to 33.6%) of girls aged 13 to 17 years in 2010 had received three doses of the HPV vaccine, and coverage was statistically significantly lower among the uninsured (14.1%, 95% CI = 9.4% to 20.6%) and in some Southern states (eg, 20.0% in Alabama [95% CI = 13.9% to 27.9%] and Mississippi [95% CI = 13.8% to 28.2%]), where cervical cancer rates were highest and recent Pap testing prevalence was the lowest.
Conclusions: The overall trends in declining cancer death rates continue. However, increases in incidence rates for some HPV-associated cancers and low vaccination coverage among adolescents underscore the need for additional prevention efforts for HPV-associated cancers, including efforts to increase vaccination coverage.
Figures
Comment in
-
Inequalities in Human Papillomavirus (HPV)-associated cancers: implications for the success of HPV vaccination.J Natl Cancer Inst. 2013 Feb 6;105(3):158-61. doi: 10.1093/jnci/djs638. Epub 2013 Jan 7. J Natl Cancer Inst. 2013. PMID: 23297040 No abstract available.
-
Re: Annual report to the nation on the status of cancer, 1975-2009, featuring the burden and trends in human papillomavirus (HPV)-associated cancers and HPV vaccination coverage levels and Re: Inequalities in human papillomavirus (HPV)-associated cancers: implications for the success of HPV vaccination.J Natl Cancer Inst. 2013 May 15;105(10):749-50. doi: 10.1093/jnci/djt083. Epub 2013 May 2. J Natl Cancer Inst. 2013. PMID: 23641042 No abstract available.
References
-
- Wingo PA, Ries LA, Rosenberg HM, et al. Cancer incidence and mortality, 1973–1995: a report card for the U.S. Cancer. 1998; 82(6):1197–1207 - PubMed
-
- Wingo PA, Ries LA, Giovino GA, et al. Annual report to the nation on the status of cancer, 1973–1996, with a special section on lung cancer and tobacco smoking. J Natl Cancer Inst. 1999; 91(8):675–690 - PubMed
-
- Ries LA, Wingo PA, Miller DS, et al. The annual report to the nation on the status of cancer, 1973–1997, with a special section on colorectal cancer. Cancer. 2000; 88(10):2398–2424 - PubMed
-
- Howe HL, Wingo PA, Thun MJ, et al. Annual report to the nation on the status of cancer (1973 through 1998), featuring cancers with recent increasing trends. J Natl Cancer Inst. 2001; 93(11):824–842 - PubMed
-
- Edwards BK, Howe HL, Ries LA, et al. Annual report to the nation on the status of cancer, 1973–1999, featuring implications of age and aging on U.S. cancer burden. Cancer. 2002; 94(10):2766–2792 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
