

Neuroimaging and other biomarkers for Alzheimer's disease: the changing landscape of early detection
- PMID: 23297785
- PMCID: PMC3955298
- DOI: 10.1146/annurev-clinpsy-050212-185535
Neuroimaging and other biomarkers for Alzheimer's disease: the changing landscape of early detection
Abstract
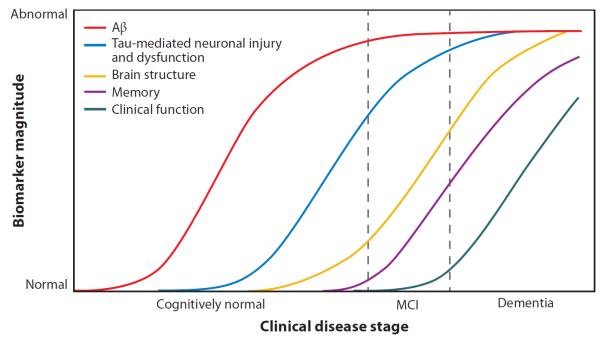
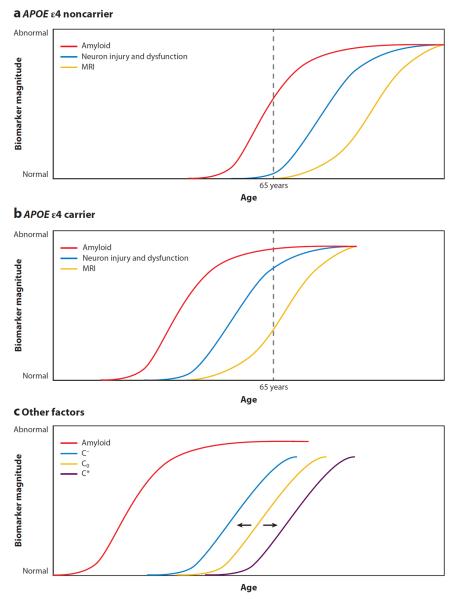
The goal of this review is to provide an overview of biomarkers for Alzheimer's disease (AD), with emphasis on neuroimaging and cerebrospinal fluid (CSF) biomarkers. We first review biomarker changes in patients with late-onset AD, including findings from studies using structural and functional magnetic resonance imaging (MRI), advanced MRI techniques (diffusion tensor imaging, magnetic resonance spectroscopy, perfusion), positron emission tomography with fluorodeoxyglucose, amyloid tracers, and other neurochemical tracers, and CSF protein levels. Next, we evaluate findings from these biomarkers in preclinical and prodromal stages of AD including mild cognitive impairment (MCI) and pre-MCI conditions conferring elevated risk. We then discuss related findings in patients with dominantly inherited AD. We conclude with a discussion of the current theoretical framework for the role of biomarkers in AD and emergent directions for AD biomarker research.
Figures
References
-
- Abdulrab K, Heun R. Subjective memory impairment. A review of its definitions indicates the need for a comprehensive set of standardised and validated criteria. Eur. Psychiatry. 2008;23:321–30. - PubMed
-
- Albert MS, DeKosky ST, Dickson D, Dubois B, Feldman HH, et al. The diagnosis of mild cognitive impairment due to Alzheimer's disease: recommendations from the National Institute on Aging—Alzheimer's Association workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimers Dement. 2011;7:270–79. - PMC - PubMed
-
- Alexander GE, Chen K, Pietrini P, Rapoport SI, Reiman EM. Longitudinal PET evaluation of cerebral metabolic decline in dementia: a potential outcome measure in Alzheimer's disease treatment studies. Am. J. Psychiatry. 2002;159:738–45. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
