

The association of clinical outcome to first-line VEGF-targeted therapy with clinical outcome to second-line VEGF-targeted therapy in metastatic renal cell carcinoma patients
- PMID: 23300029
- PMCID: PMC4144038
- DOI: 10.1007/s11523-012-0252-7
The association of clinical outcome to first-line VEGF-targeted therapy with clinical outcome to second-line VEGF-targeted therapy in metastatic renal cell carcinoma patients
Abstract
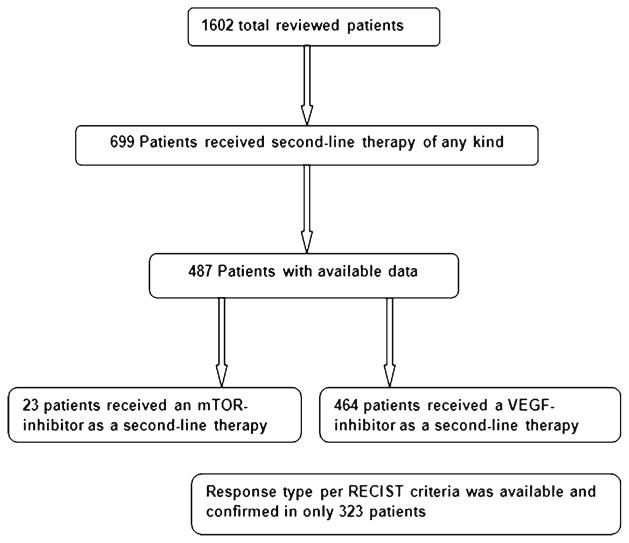
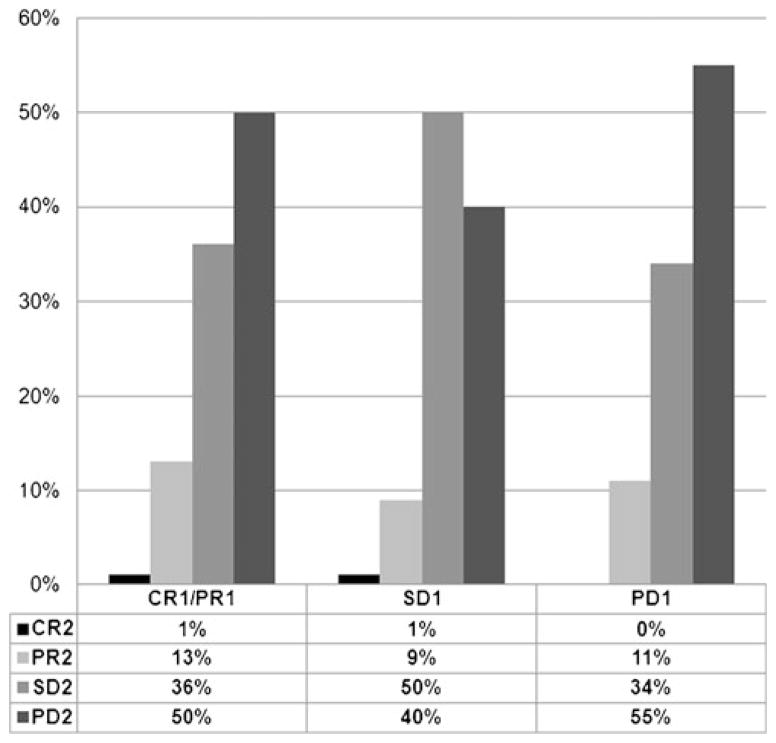
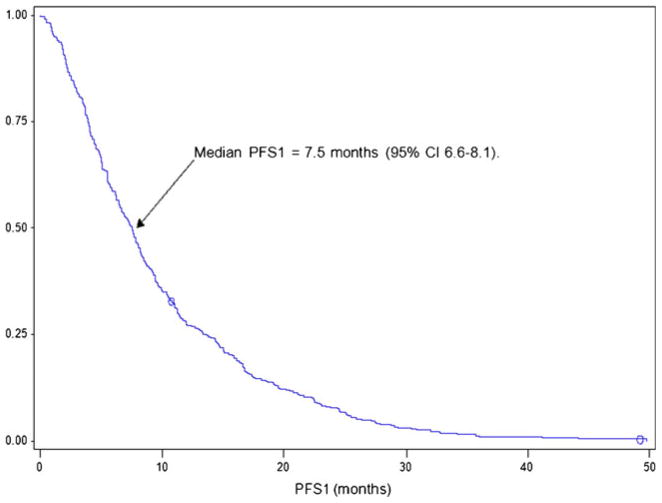
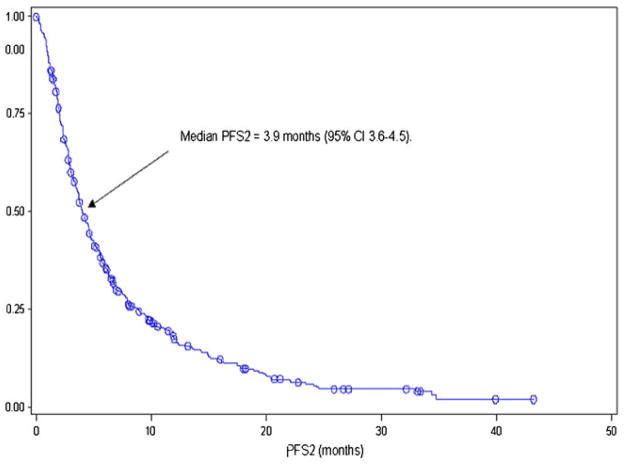
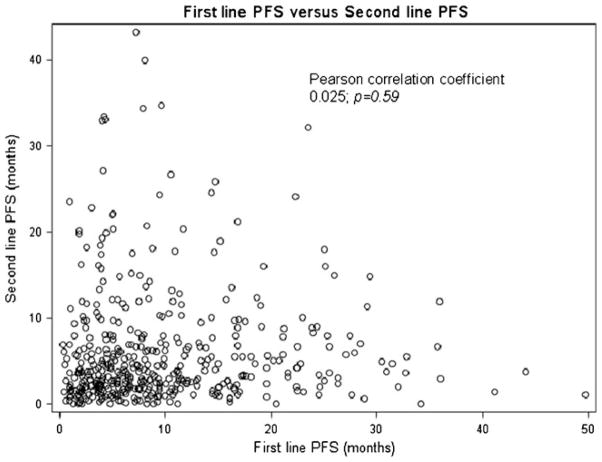
There are many active drugs to treat metastatic renal cell carcinoma (mRCC) patients who progress through their first-line vascular endothelial growth factor (VEGF) inhibitor. Many clinicians choose a second-line VEGF inhibitor based on the type of response to first-line VEGF inhibitor, without data supporting this practice. This study was conducted to determine the association of response to second-line VEGF inhibitor with response to first-line VEGF inhibitor. All mRCC patients in participating centers of the International mRCC Database Consortium who were treated from January 2004 through June 2011 with a second-line VEGF inhibitor after failure of a different first-line VEGF inhibitor were retrospectively identified. The primary outcome is objective response rate (ORR) and the secondary outcome is progression-free survival (PFS) in each line of therapy. Of 1,602 total database patients, 464 patients received a first- and second-line VEGF inhibitor. The ORR to first-line therapy was 22%, and the ORR to second-line therapy was 11%. The ORR to second-line therapy was not different among patients achieving partial response versus stable disease versus progressive disease to first-line therapy (14% vs. 10% vs. 11%, respectively; chi-squared trend test p=0.17). The median PFS on first-line VEGF-targeted therapy was 7.5 months (95% CI, 6.6-8.1), and the median PFS on second-line VEGF inhibitor was 3.9 months (95% CI, 3.6-4.5). There was no correlation between first-line and second-line PFS (Pearson correlation coefficient 0.025; p=0.59). The clinical response to a second-line VEGF inhibitor is not dependent on response to the first-line VEGF-inhibitor. Further studies are needed to define clinical parameters that predict response to second-line therapy to optimize the sequence of VEGF-targeted therapy in metastatic RCC patients.
Conflict of interest statement
Figures
References
-
- Escudier B, Bellmunt J, Negrier S, et al. Phase III trial of bevacizumab plus interferon alfa-2a in patients with metastatic renal cell carcinoma (AVOREN): final analysis of overall survival. J Clin Oncol. 2010;28(13):2144–2150. - PubMed
-
- Al-Marrawi MY, Rini BI. Pazopanib for the treatment of renal cancer. Expert Opin Pharmacother. 2011;12(7):1171–1189. - PubMed
-
- Sternberg CN, Davis ID, Mardiak J, et al. Pazopanib in locally advanced or metastatic renal cell carcinoma: results of a randomized phase III trial. J Clin Oncol. 2010;28(6):1061–1068. - PubMed
-
- Escudier B, Szczylik C, Hutson TE, et al. Randomized phase II trial of first-line treatment with sorafenib versus interferon alfa-2a in patients with metastatic renal cell carcinoma. J Clin Oncol. 2009;27(8):1280–1289. Erratum in J Clin Oncol. 2009 May 1; 27(13):2305. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
