

Epidemiology of falls and osteoporotic fractures: a systematic review
- PMID: 23300349
- PMCID: PMC3536355
- DOI: 10.2147/CEOR.S38721
Epidemiology of falls and osteoporotic fractures: a systematic review
Abstract
Background and methods: Fractures in elderly populations result from the combination of falls and osteoporosis. We report a systematic review of studies indexed in PubMed reporting annual rates of low-trauma falls and associated osteoporotic fractures among older community-dwelling people (age ≥ 50 years). An osteoporotic fracture was defined as either a fracture resulting from a low-impact fall in subjects with clinical osteoporosis, a fall resulting in an investigator-defined osteoporotic fracture, or a fall resulting in a low-trauma fracture. Rates are presented using descriptive statistics. Meta-analysis was conducted for statistically homogeneous data sets.
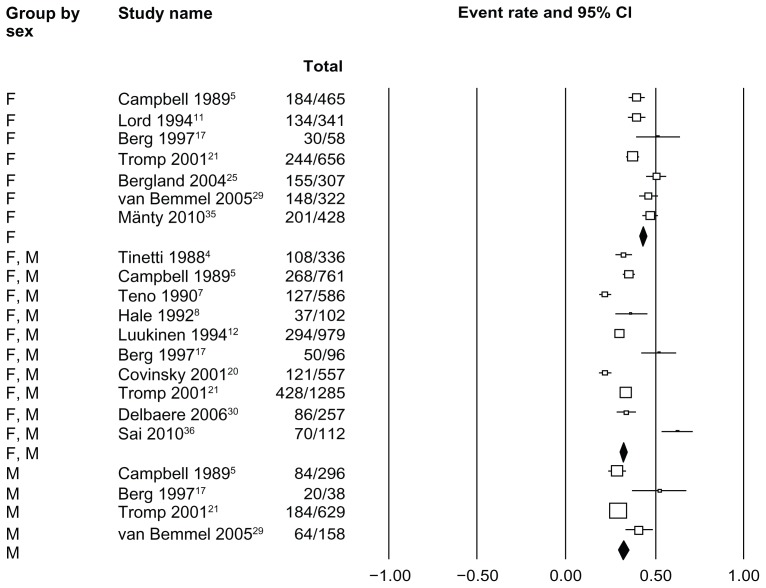
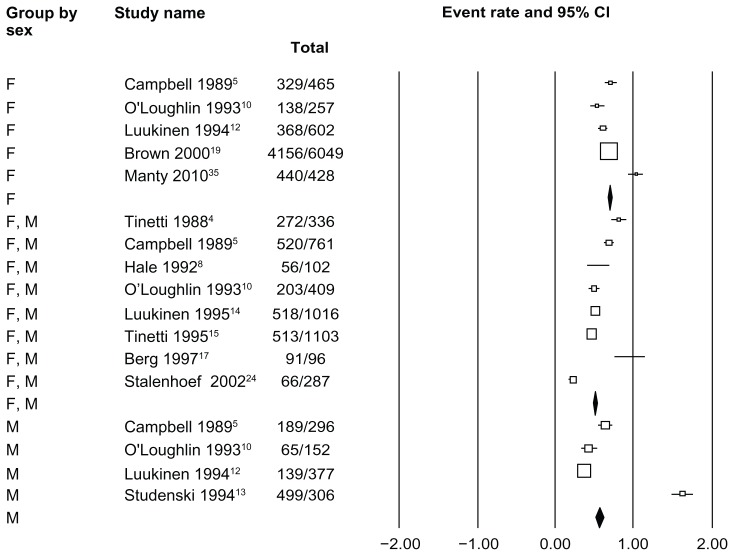
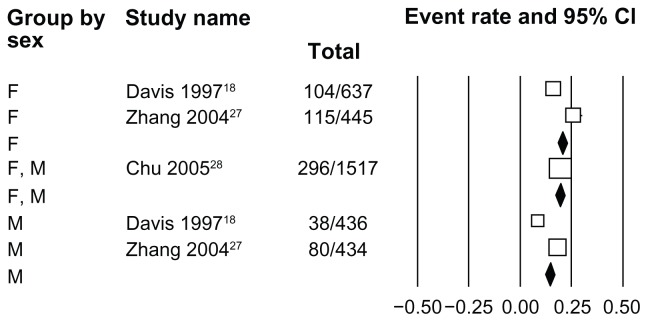
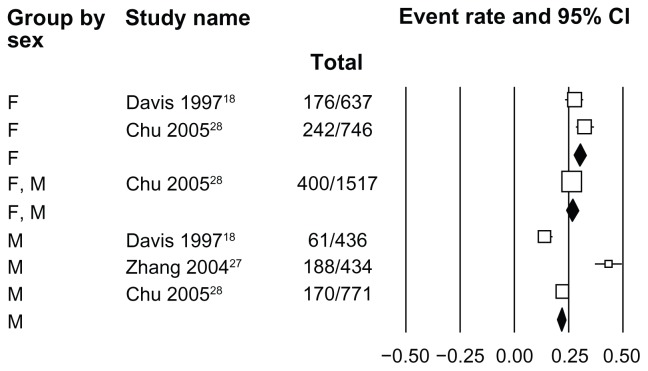
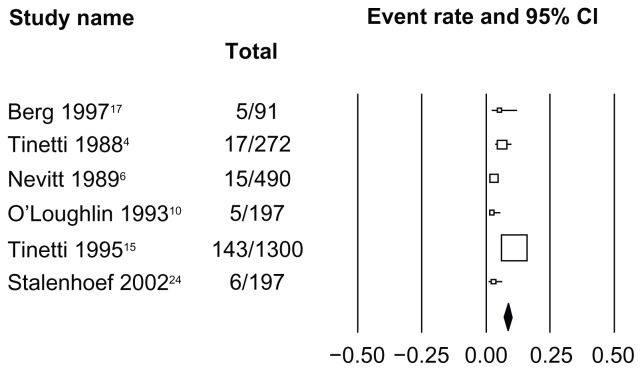
Results: The median (range) annual fall prevalence rates (median proportion of people who experienced one or more falls during the past year) for cohorts of women and men (10 determinations), women alone (seven determinations), and men alone (four determinations) were, respectively, 0.334 (0.217-0.625), 0.460 (0.372-0.517), and 0.349 (0.284-0.526). In studies that reported fall prevalence rates for Western men and women separately (four determinations), the pooled risk ratio (95% confidence interval [CI]) for men versus women was 0.805 (95% CI 0.721-0.900). The ranges of fall prevalence rates in East Asian women (two studies) and East Asian men (two studies) were, respectively, 0.163-0.258 and 0.087-0.184. The risk ratio (95% CI) for fall prevalence in East Asian men versus women was 0.634 (0.479-0.838) in studies (two determinations) reporting results for East Asian men and women separately. In cohorts of Western women and men (five determinations), the pooled rate (95% CI) of low-impact falls resulting in fractures was 0.041 (0.031-0.054). The proportion of low-trauma fractures attributable to falls among the Western community-dwelling elderly was within the range of 0.860-0.950 for fractures at all sites or the hip (five determinations). A range of 0.716-0.924 of all fractures were osteoporotic (eight determinations).
Conclusion: Fall rates are higher in women than in men in Western community-dwelling populations and lower in East Asian populations. Extrapolated to the US population, the statistics imply that low-impact falls cause approximately 0.53 million osteoporotic fractures annually among the US community-dwelling elderly.
Keywords: accidental falls; aged; bone density; fractures; osteoporosis.
Figures
References
-
- Geusens P, Autier P, Boonen S, Vanhoof J, Declerck K, Raus J. The relationship among history of falls, osteoporosis, and fractures in postmenopausal women. Arch Phys Med Rehabil. 2002;83(7):903–906. - PubMed
-
- Rubenstein LZ, Josephson KR. The epidemiology of falls and syncope. Clin Geriatr Med. 2002;18(2):141–158. - PubMed
-
- Ganz DA, Bao Y, Shekelle PG, Rubenstein LZ. Will my patient fall? JAMA. 2007;297(1):77–86. - PubMed
-
- Tinetti ME, Speechley M, Ginter SF. Risk factors for falls among elderly persons living in the community. N Engl J Med. 1988;319(26):1701–1707. - PubMed
-
- Campbell AJ, Borrie MJ, Spears GF. Risk factors for falls in a community-based prospective study of people 70 years and older. J Gerontol. 1989;44(4):M112–M117. - PubMed
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
