

Clinical, imaging, and pathological heterogeneity of the Alzheimer's disease syndrome
- PMID: 23302773
- PMCID: PMC3580331
- DOI: 10.1186/alzrt155
Clinical, imaging, and pathological heterogeneity of the Alzheimer's disease syndrome
Abstract
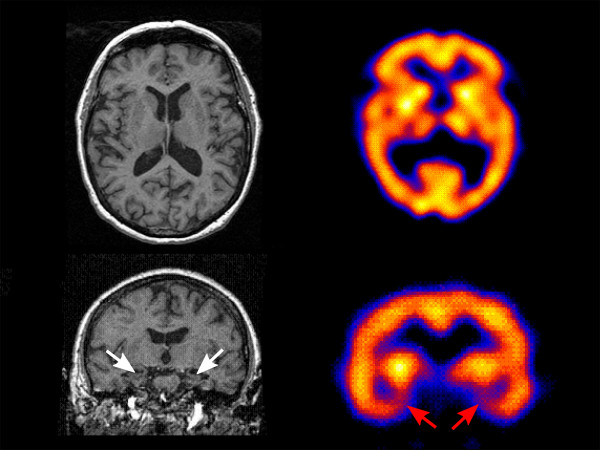
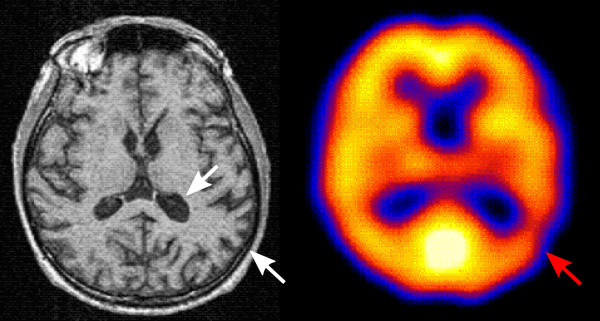
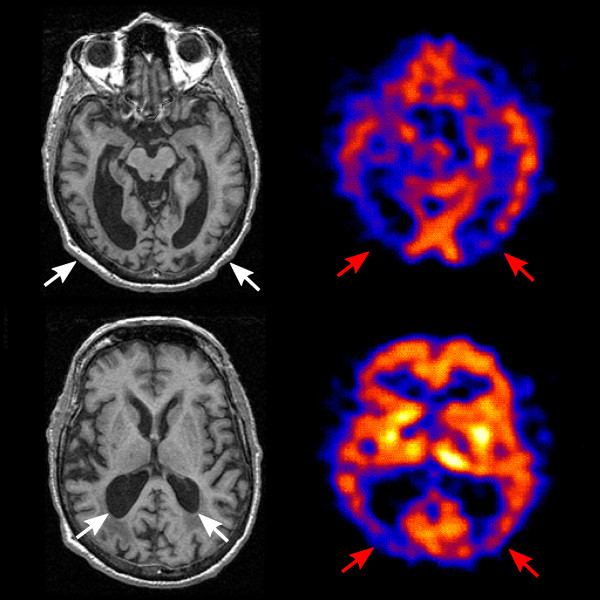
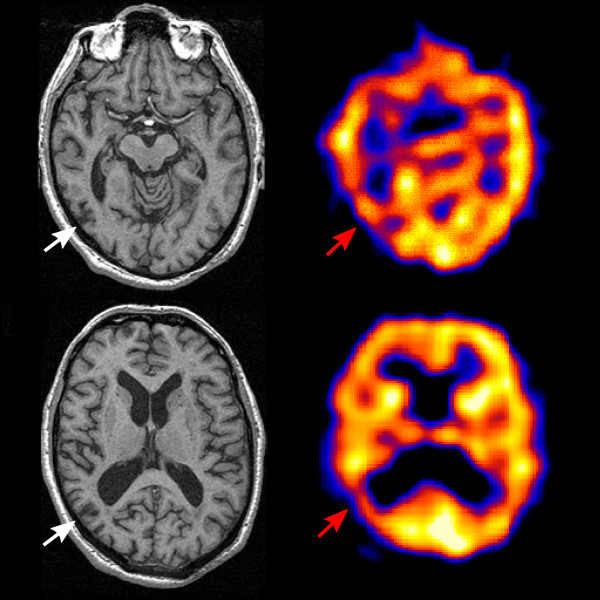
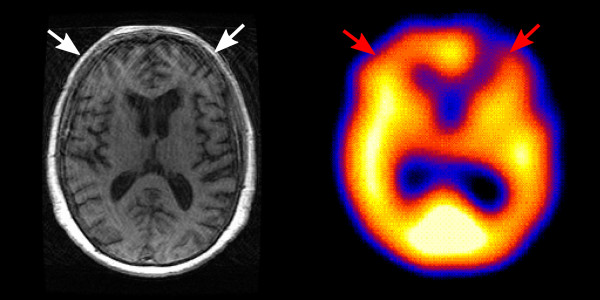
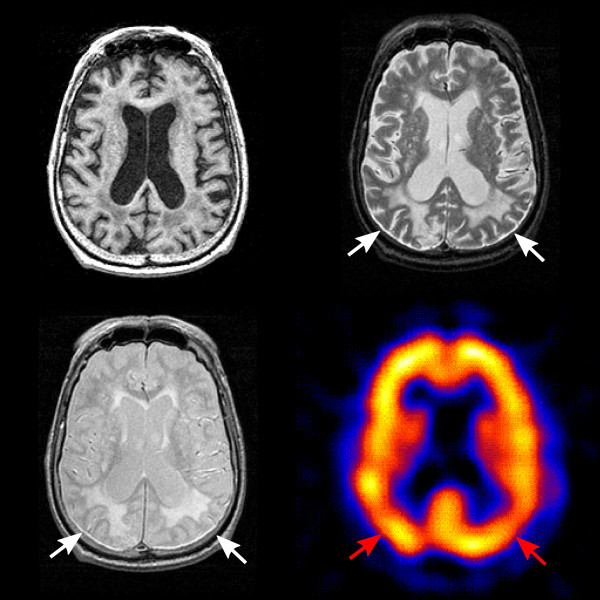
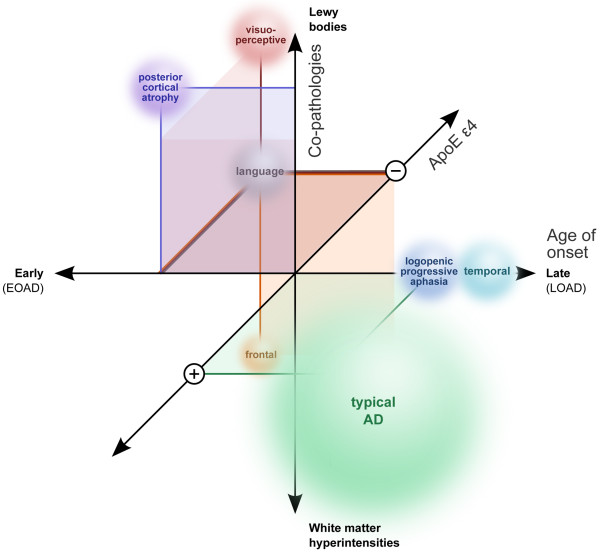
With increasing knowledge of clinical in vivo biomarkers and the pathological intricacies of Alzheimer's disease (AD), nosology is evolving. Harmonized consensus criteria that emphasize prototypic illness continue to develop to achieve diagnostic clarity for treatment decisions and clinical trials. However, it is clear that AD is clinically heterogeneous in presentation and progression, demonstrating variable topographic distributions of atrophy and hypometabolism/hypoperfusion. AD furthermore often keeps company with other conditions that may further nuance clinical expression, such as synucleinopathy exacerbating executive and visuospatial dysfunction and vascular pathologies (particularly small vessel disease that is increasingly ubiquitous with human aging) accentuating frontal-dysexecutive symptomatology. That some of these atypical clinical patterns recur may imply the existence of distinct AD variants. For example, focal temporal lobe dysfunction is associated with a pure amnestic syndrome, very slow decline, with atrophy and neurofibrillary tangles limited largely to the medial temporal region including the entorhinal cortex. Left parietal atrophy and/or hypometabolism/hypoperfusion are associated with language symptoms, younger age of onset, and faster rate of decline - a potential 'language variant' of AD. Conversely, the same pattern but predominantly affecting the right parietal lobe is associated with a similar syndrome but with visuospatial symptoms replacing impaired language function. Finally, the extremely rare frontal variant is associated with executive dysfunction out of keeping with degree of memory decline and may have prominent behavioural symptoms. Genotypic differences may underlie some of these subtypes; for example, absence of apolipoprotein E e4 is often associated with atypicality in younger onset AD. Understanding the mechanisms behind this variability merits further investigation, informed by recent advances in imaging techniques, biomarker assays, and quantitative pathological methods, in conjunction with standardized clinical, functional, neuropsychological and neurobehavioral evaluations. Such an understanding is needed to facilitate 'personalized AD medicine', and eventually allow for clinical trials targeting specific AD subtypes. Although the focus legitimately remains on prototypic illness, continuing efforts to develop disease-modifying therapies should not exclude the rarer AD subtypes and common comorbid presentations, as is currently often the case. Only by treating them as well can we address the full burden of this devastating dementia syndrome.
Figures
References
-
- McKhann G, Drachman D, Folstein M, Katzman R, Price D, Stadlan EM. Clinical diagnosis of Alzheimer's disease: report of the NINCDS-ADRDA Work Group under the auspices of Department of Health and Human Services Task Force on Alzheimer's Disease. Neurology. 1984;34:939–944. doi: 10.1212/WNL.34.7.939. - DOI - PubMed
-
- McKhann GM, Knopman DS, Chertkow H, Hyman BT, Jack CR Jr, Kawas CH, Klunk WE, Koroshetz WJ, Manly JJ, Mayeux R, Mohs RC, Morris JC, Rossor MN, Scheltens P, Carrillo MC, Thies B, Weintraub S, Phelps CH. The diagnosis of dementia due to Alzheimer's disease: recommendations from the National Institute on Aging-Alzheimer's Association workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimers Dement. 2011;7:263–269. doi: 10.1016/j.jalz.2011.03.005. - DOI - PMC - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
