

Intermittent self catheterisation with hydrophilic, gel reservoir, and non-coated catheters: a systematic review and cost effectiveness analysis
- PMID: 23303886
- PMCID: PMC3541473
- DOI: 10.1136/bmj.e8639
Intermittent self catheterisation with hydrophilic, gel reservoir, and non-coated catheters: a systematic review and cost effectiveness analysis
Abstract
Objective: To determine the most effective and cost effective type of catheter for patients performing intermittent self catheterisation in the community.
Design: Systematic review and meta-analysis. Results were incorporated into a probabilistic Markov model to compare lifetime costs and quality adjusted life years (QALYs).
Data sources: We searched Medline, Embase, and Cochrane and Cinahl databases from 2002 to 18 April 2011 to identify studies comparing hydrophilic, gel reservoir, and non-coated intermittent catheters. Earlier guidelines were used to identify papers published before 2002. To capture studies comparing clean and sterile non-coated intermittent self catheterisation, each database was searched from its date of inception to 18 April 2011.
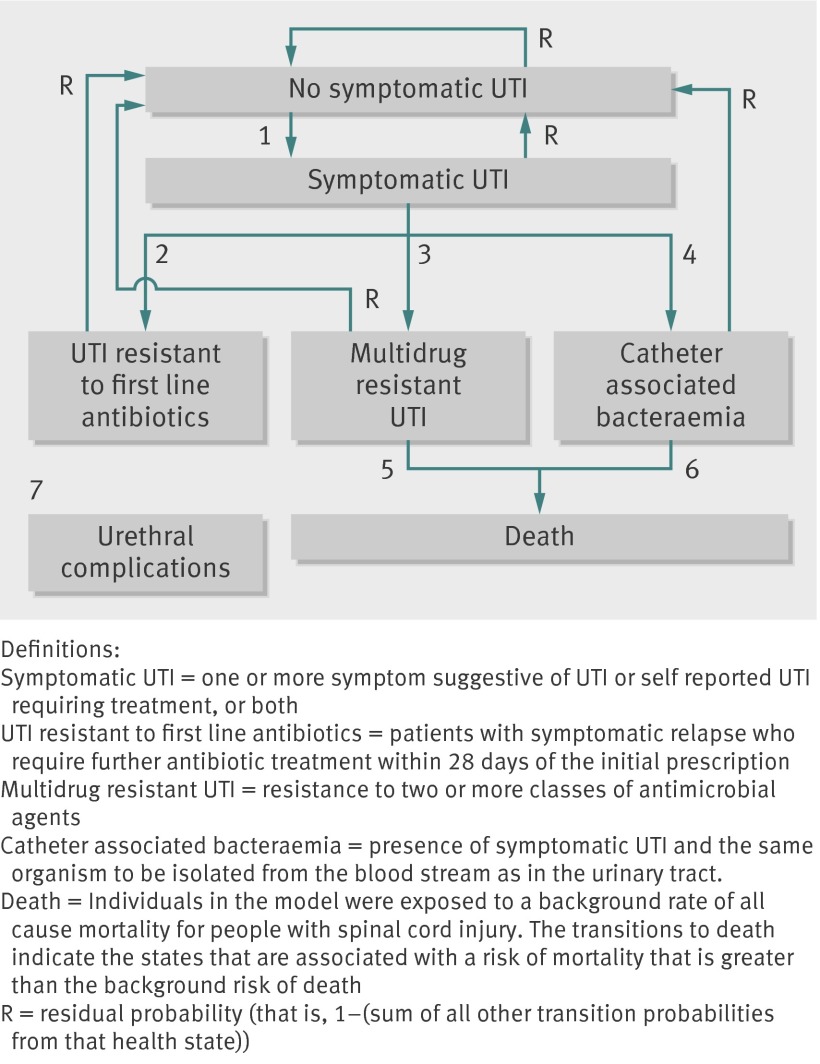
Main outcome measures: Clinical outcomes included symptomatic urinary tract infection (UTI), bacteraemia, mortality, patient preference or comfort, and number of catheters used. The economic model included downstream complications of UTI and cost effectiveness was calculated as incremental cost per QALY gained.
Results: Eight studies were included in the systematic review. Most were conducted in patients with spinal cord injuries, and most of the included patients were men. People using gel reservoir and hydrophilic catheters were significantly less likely to report one or more UTIs compared with sterile non-coated catheters (absolute effect for gel reservoir = 149 fewer per 1000 (95% confidence interval -7 to 198), P=0.04; absolute effect for hydrophilic = 153 fewer per 1000 (-8 to 268), P=0.04). However, there was no difference between hydrophilic and sterile non-coated catheters when outcomes were measured as mean monthly UTIs (mean difference = 0.01 (-0.11 to 0.09), P=0.84) or total UTIs at 1 year (mean difference = 0.18 (-0.50 to 0.86), P=0.60). There was little difference in the incidence of one or more UTIs for people using clean versus sterile non-coated catheters (absolute effect = 12 fewer per 1000 (-134 to 146), P=0.86). Although the most effective, gel reservoir catheters cost >£54,350 per QALY gained and are therefore not cost effective compared with clean non-coated self catheterisation.
Conclusion: The type of catheter used for intermittent self catheterisation seems to make little difference to the risk of symptomatic UTI. Given large differences in resource use, clean non-coated catheters are most cost effective. However, because of limitations and gaps in the evidence base and the designation of non-coated catheters as single use devices, we recommend a precautionary principle should be adopted and that patients should be offered a choice between hydrophilic and gel reservoir catheters.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures


Comment in
-
Re: Intermittent Self Catheterisation with Hydrophilic, Gel Reservoir, and Non-Coated Catheters: A Systematic Review and Cost Effectiveness Analysis.J Urol. 2015 Dec;194(6):1644. doi: 10.1016/j.juro.2015.09.054. Epub 2015 Sep 21. J Urol. 2015. PMID: 26582673 No abstract available.
References
-
- Plowman R, Graves N, Esquivel J, Roberts JA. An economic model to assess the cost and benefits of the routine use of silver alloy coated urinary catheters to reduce the risk of urinary tract infections in catheterized patients. J Hosp Infect 2001;48:33-42. - PubMed
-
- Plowman R, Graves N, Griffin M, Roberts JA, Swan AV, Cookson B, et al. The socio-economic burden of hospital acquired infection: executive summary. Health Protection Agency;1999.
-
- Pilloni S, Krhut J, Mair D, Madersbacher H, Kessler TM. Intermittent catheterisation in older people: a valuable alternative to an indwelling catheter? Age Aging 2005;34:34-60. - PubMed
-
- Larsen LD, Chamberlin DA, Khonsari F, Ahlering TE. Retrospective analysis of urologic complications in male patients with spinal cord injury managed with and without indwelling urinary catheters. Urology 1997;50:418-22. - PubMed
-
- Wyndaele JJ. Complications of intermittent catheterization: their prevention and treatment. Spinal Cord 2002;40:536-41. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous