

Learning to predict post-hospitalization VTE risk from EHR data
- PMID: 23304314
- PMCID: PMC3540493
Learning to predict post-hospitalization VTE risk from EHR data
Abstract
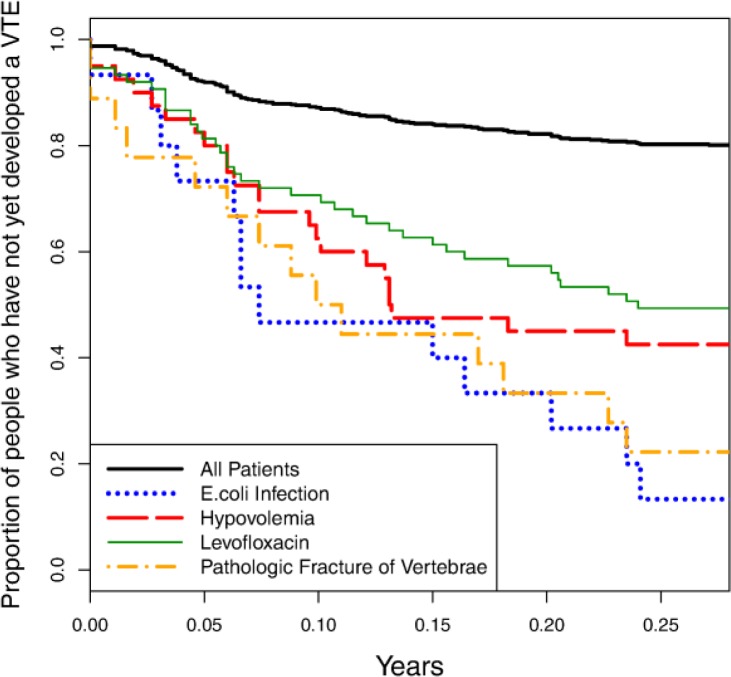
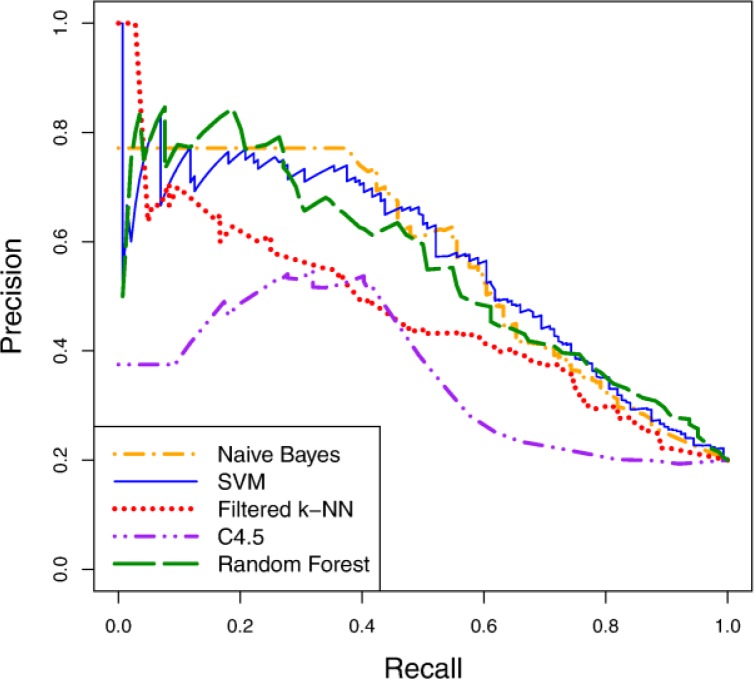
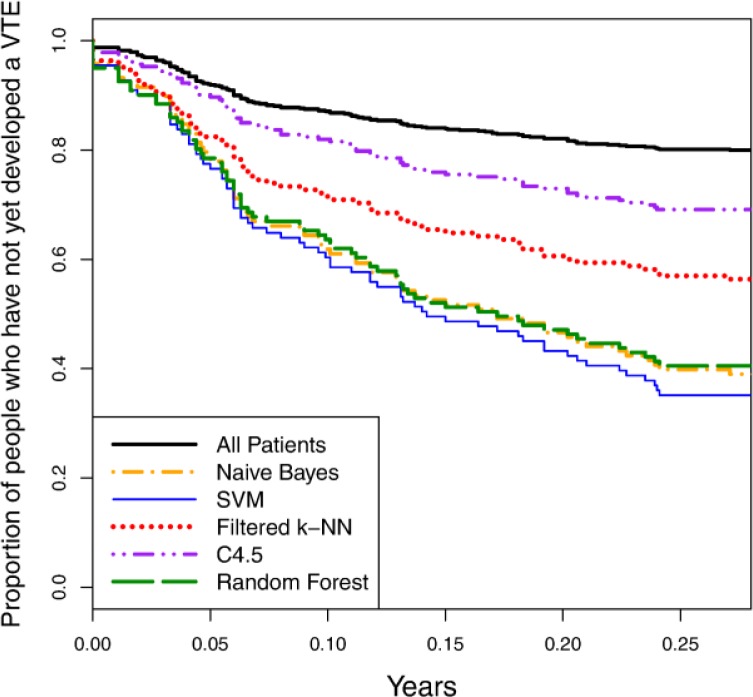
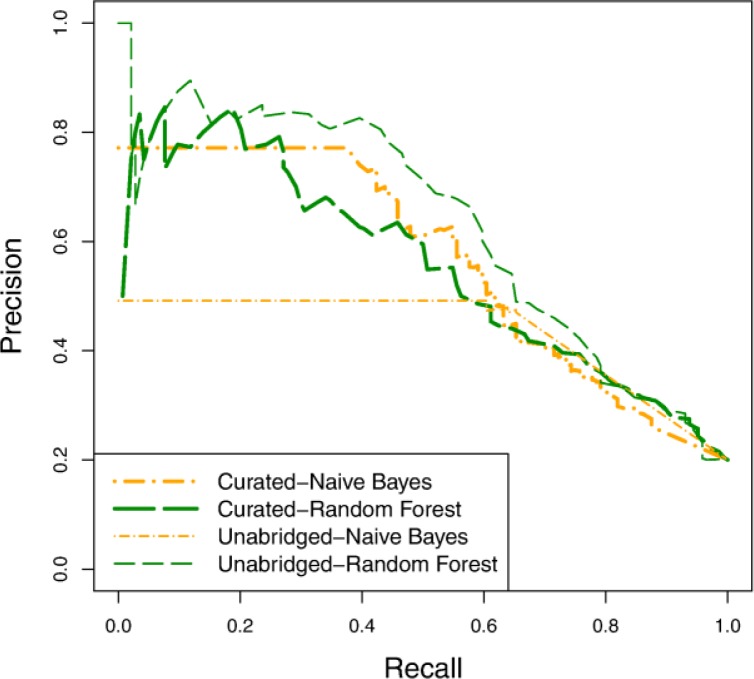
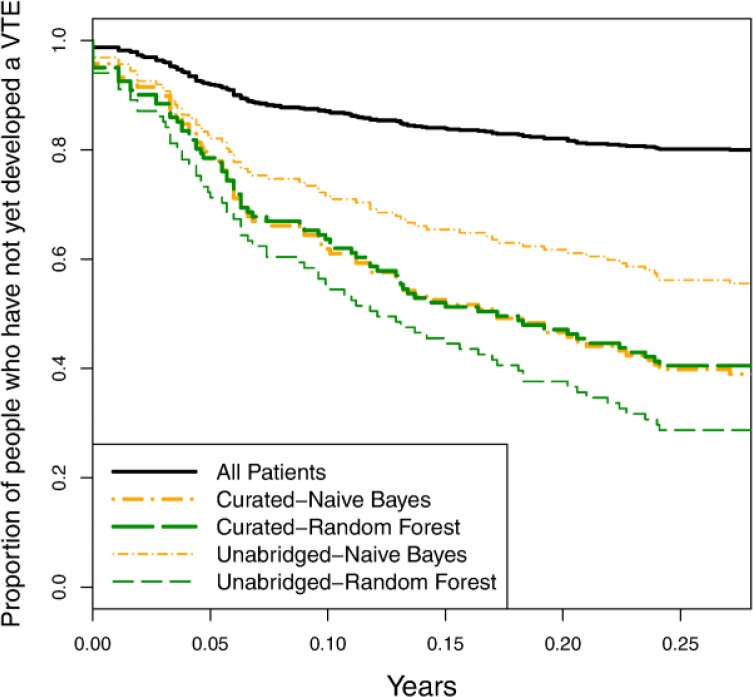
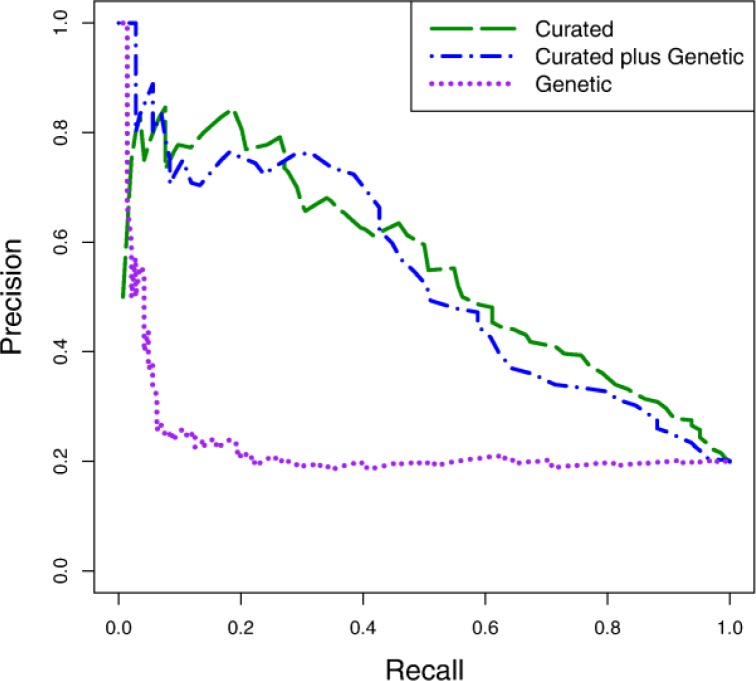
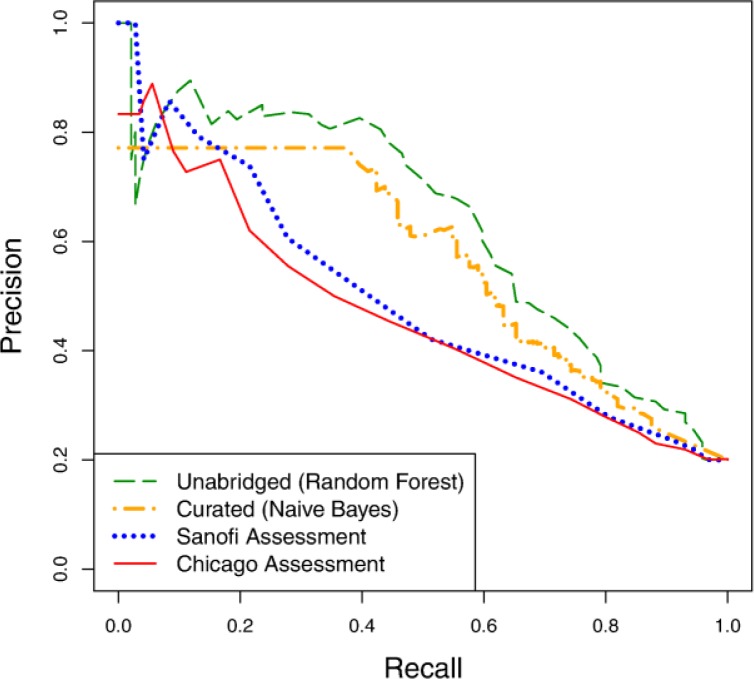
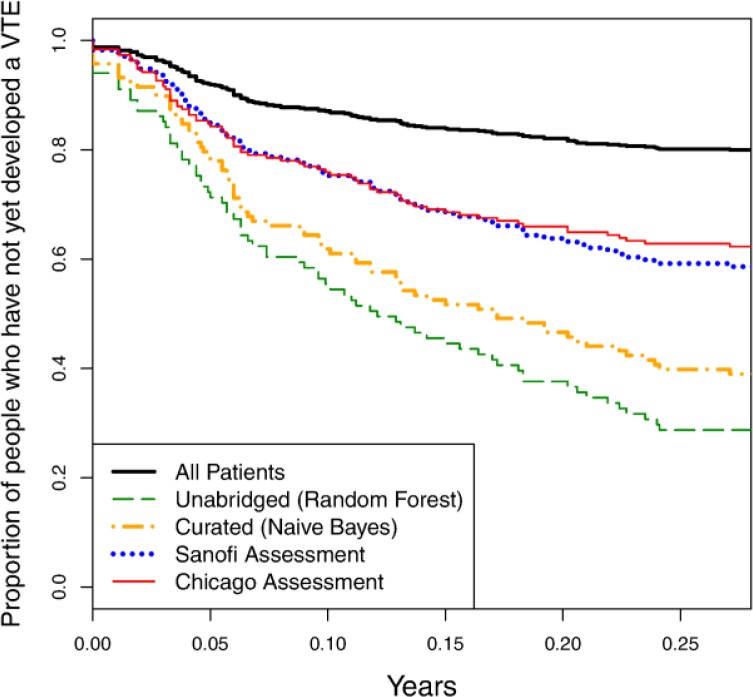
We consider the task of predicting which patients are most at risk for post-hospitalization venothromboembolism (VTE) using information automatically elicited from an EHR. Given a set of cases and controls, we use machine-learning methods to induce models for making these predictions. Our empirical evaluation of this approach offers a number of interesting and important conclusions. We identify several risk factors for VTE that were not previously recognized. We show that machine-learning methods are able to induce models that identify high-risk patients with accuracy that exceeds previously developed scoring models for VTE. Additionally, we show that, even without having prior knowledge about relevant risk factors, we are able to learn accurate models for this task.
Figures
Similar articles
-
Prediction of hospitalization due to heart diseases by supervised learning methods.Int J Med Inform. 2015 Mar;84(3):189-97. doi: 10.1016/j.ijmedinf.2014.10.002. Epub 2014 Oct 16. Int J Med Inform. 2015. PMID: 25497295 Free PMC article.
-
A gradient boosting tree model for multi-department venous thromboembolism risk assessment with imbalanced data.J Biomed Inform. 2022 Oct;134:104210. doi: 10.1016/j.jbi.2022.104210. Epub 2022 Sep 16. J Biomed Inform. 2022. PMID: 36122879
-
Prediction of venous thromboembolism using semantic and sentiment analyses of clinical narratives.Comput Biol Med. 2018 Mar 1;94:1-10. doi: 10.1016/j.compbiomed.2017.12.026. Epub 2018 Jan 3. Comput Biol Med. 2018. PMID: 29353160
-
Scoring Systems for Estimating Risk of Venous Thromboembolism in Hospitalized Medical Patients.Semin Thromb Hemost. 2017 Jul;43(5):460-468. doi: 10.1055/s-0036-1597901. Epub 2017 Feb 6. Semin Thromb Hemost. 2017. PMID: 28166598 Review.
-
Risk Assessment Scores for Cancer-Associated Venous Thromboembolic Disease.Semin Thromb Hemost. 2017 Jul;43(5):469-478. doi: 10.1055/s-0036-1597281. Epub 2017 Mar 6. Semin Thromb Hemost. 2017. PMID: 28264198 Review.
Cited by
-
Artificial Intelligence-Based Prediction of Lower Extremity Deep Vein Thrombosis Risk After Knee/Hip Arthroplasty.Clin Appl Thromb Hemost. 2023 Jan-Dec;29:10760296221139263. doi: 10.1177/10760296221139263. Clin Appl Thromb Hemost. 2023. PMID: 36596268 Free PMC article.
-
Validated risk prediction models for outcomes of acute kidney injury: a systematic review.BMC Nephrol. 2023 May 9;24(1):133. doi: 10.1186/s12882-023-03150-0. BMC Nephrol. 2023. PMID: 37161365 Free PMC article.
-
Opportunities and challenges in developing risk prediction models with electronic health records data: a systematic review.J Am Med Inform Assoc. 2017 Jan;24(1):198-208. doi: 10.1093/jamia/ocw042. Epub 2016 May 17. J Am Med Inform Assoc. 2017. PMID: 27189013 Free PMC article.
-
Cost-sensitive Active Learning for Phenotyping of Electronic Health Records.AMIA Jt Summits Transl Sci Proc. 2019 May 6;2019:829-838. eCollection 2019. AMIA Jt Summits Transl Sci Proc. 2019. PMID: 31259040 Free PMC article.
-
Risk factors for deep vein thrombosis of the lower extremity after total hip arthroplasty.BMC Surg. 2024 Sep 11;24(1):256. doi: 10.1186/s12893-024-02561-6. BMC Surg. 2024. PMID: 39261801 Free PMC article.
References
-
- Edelsberg J, Hagiwara M, Taneja C, Oster G. Risk of venous thromboembolism among hospitalized medically ill patients. American Journal of Health-System Pharmacy. 2006;63:S16–S22. - PubMed
-
- Anderson FA, Spencer FA. Risk factors for venous thromboembolism. Circulation. 2003;107(23 Suppl 1):I9–I16. - PubMed
-
- White RH. The epidemiology of venous thromboembolism. Circulation. 2003;107(Suppl 1):I4–I8. - PubMed
-
- U.S. Department of Health and Human Services . The Surgeon General’s call to action to prevent deep vein thrombosis and pulmonary embolism. 2008. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources