

Catamenial pneumothorax: a rare entity? Report of 5 cases and review of the literature
- PMID: 23304438
- PMCID: PMC3537379
- DOI: 10.3978/j.issn.2072-1439.2012.s006
Catamenial pneumothorax: a rare entity? Report of 5 cases and review of the literature
Abstract
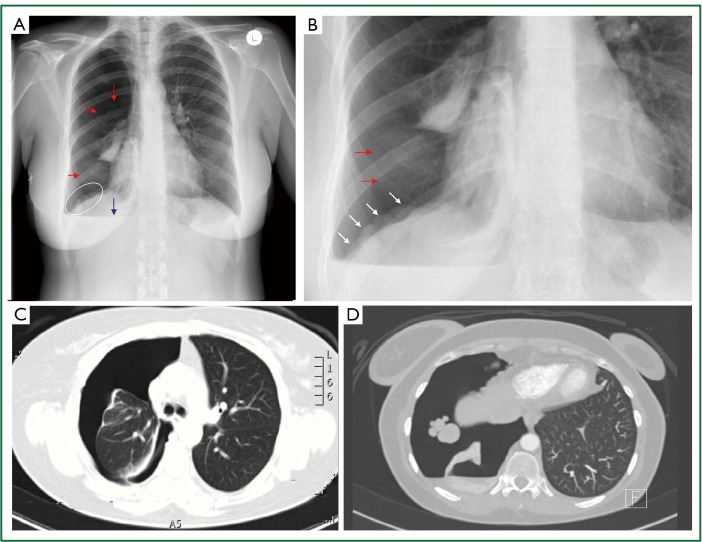
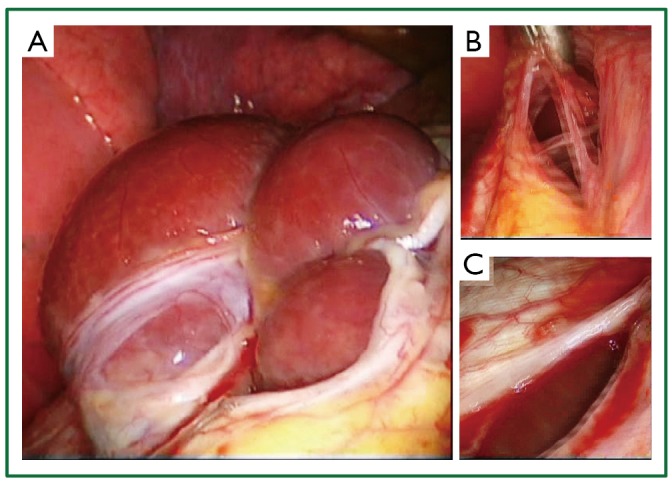
Objective: Spontaneous recurrent pneumothorax during menstruation is reported as catamenial pneumothorax. It is encountered in 3-6% of spontaneous pneumothorax cases among menstruating women. The percentage among women referred for surgery is significantly higher (25-30%). Although it usually involves the right-side (85-95%) it can be left-sided or bilateral. It is associated with diaphragmatic perforations and/or thoracic endometriosis. There is pelvic endometriosis in up to 30-51% of cases. The lesions that are not always found may present as small or larger holes at the central tendon of the diaphragm, as red, blueberry, brown spots or larger nodules at the diaphragm, the visceral or parietal pleura. Lesion histology may reveal endometriosis. We present 5 cases of catamenial pneumothorax treated surgically during the last 6 years.
Patients and methods: Five women, with a mean age of 34+/-9.9 years (median 38, range, 19-45 years) presented with right-sided recurrent catamenial pneumothorax. In 3 patients diaphragmatic perforation(s) were found; perforation suturing (n=1), and diaphragmatic plication reinforced with bovine pericardial patch (n=1) were performed. All patients underwent atypical resection of upper and/or middle lobe segments of lung parenchyma that appeared abnormal (haemorrhagic/emphysematous or blebs). Four patients underwent pleurodesis and 1 patient underwent pleurectomy. Four interventions were performed through video assisted thoracoscopic surgery, while diaphragmatic plication was performed through a video assisted mini-thoracotomy. Histology did not reveal endometriosis tissue.
Results: The postoperative course was uneventful. The patients were extubated in theatre and were discharged home at a mean of 7+/-4 days (median 6 days, range, 4-14 days). Two of them received hormonal therapy [Gonadotropin Releasing Hormone (GnRH) analogue] postoperatively. At a follow-up of 14.16 patient-years (mean 2.83+/-1.08 years, range, 1.33-3.83 years) there was recurrence, 6.5 months postoperatively, in one patient that had not undergone closure of a tiny diaphragmatic hole and had not received hormonal treatment postoperatively. She was treated medically (amenorrhea for 6 months with GnRH analogue) and had no further recurrences (in 3.3 years).
Conclusions: Surgery is the treatment of choice of catamenial pneumothorax. It should aim to complete management of all lesions. The most common complication is recurrence. Early diagnosis and multidisciplinary treatment including hormonal therapy may be beneficial in high risk patients.
Keywords: Catamenial pneumothorax; thoracic endometriosis; video-assisted thoracoscopic surgery.
Figures





References
-
- Alifano M, Vénissac N, Mouroux J.Recurrent pneumothorax associated with thoracic endometriosis. Surg Endosc 2000;14:680. - PubMed
-
- Alifano M, Roth T, Broët SC, et al. Catamenial pneumothorax: a prospective study. Chest 2003;124:1004-8 - PubMed
-
- Alifano M, Jablonski C, Kadiri H, et al. Catamenial and noncatamenial, endometriosis-related or nonendometriosis-related pneumothorax referred for surgery. Am J Respir Crit Care Med 2007;176:1048-53 - PubMed
-
- Alifano M.Catamenial pneumothorax. Curr Opin Pulm Med 2010;16:381-6 - PubMed
-
- Rousset-Jablonski C, Alifano M, Plu-Bureau G, et al. Catamenial pneumothorax and endometriosis-related pneumothorax: clinical features and risk factors. Hum Reprod 2011;26:2322-9 - PubMed
LinkOut - more resources
Full Text Sources