

Resection of a giant bilateral retrovascular intrathoracic goiter causing severe upper airway obstruction, 2 years after subtotal thyroidectomy: a case report and review of the literature
- PMID: 23304440
- PMCID: PMC3537381
- DOI: 10.3978/j.issn.2072-1439.2012.s004
Resection of a giant bilateral retrovascular intrathoracic goiter causing severe upper airway obstruction, 2 years after subtotal thyroidectomy: a case report and review of the literature
Abstract
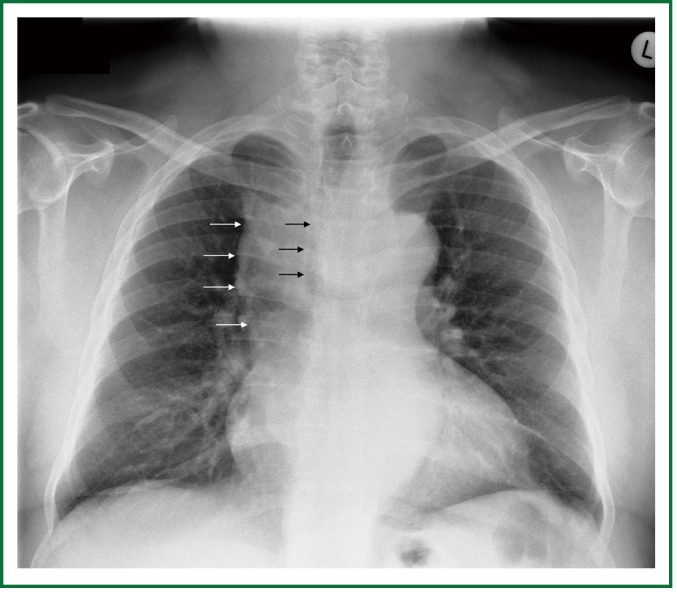
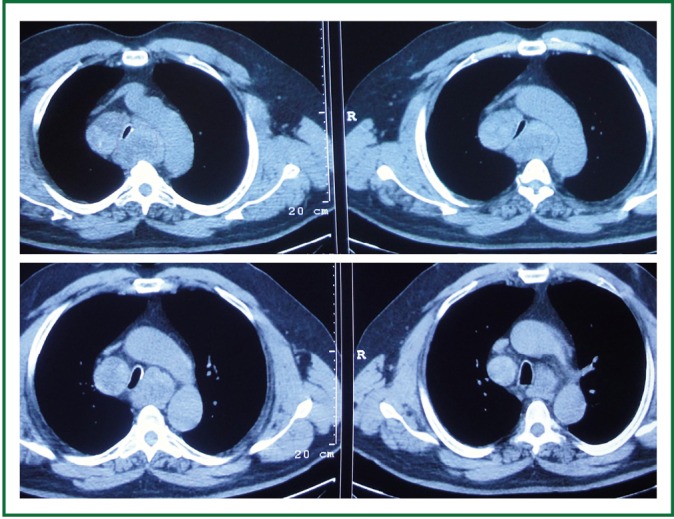
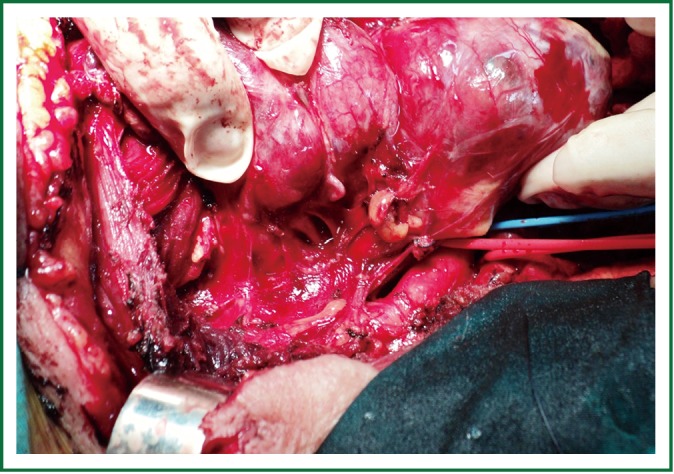
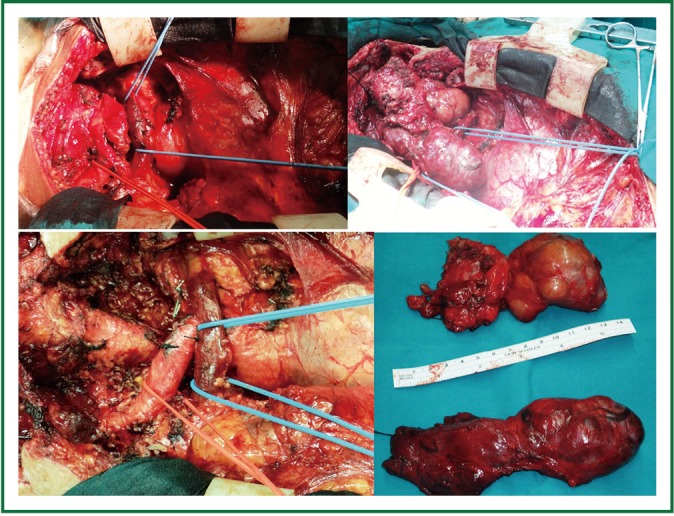
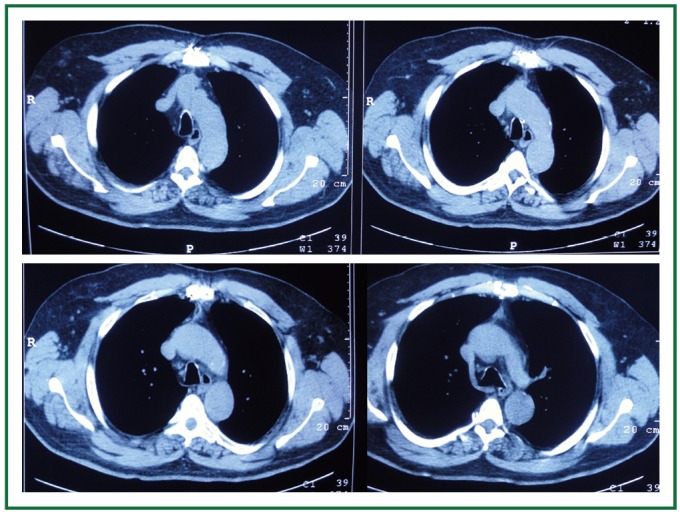
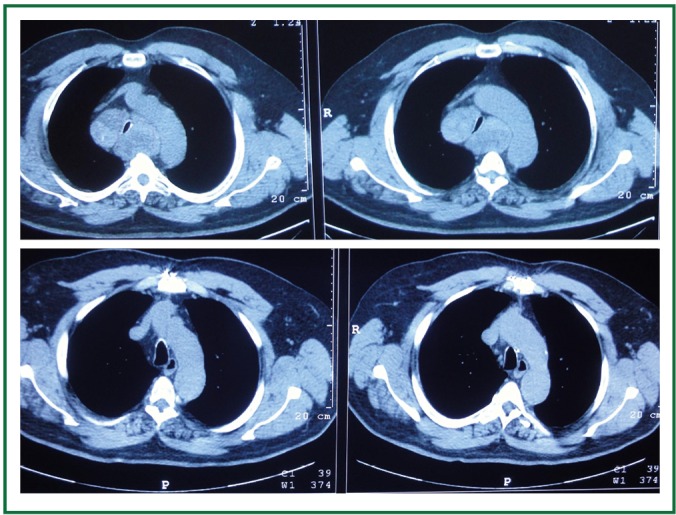
The intrathoracic (or substernal) goiter is more often benign; but it can be malignant in 2-22% of patients. There is history of prior thyroid surgery in 10% to more than 30% of patients. Intrathoracic goiters cause adjacent structure compression more frequently than the cervical goiters, due to the limited space of the thoracic cage. Compression of trachea, oesophagus, vascular and neural structures may cause dyspnoea, dysphagia, superior vena cava syndrome, subclavian vein thrombosis, hoarseness, and Horner's syndrome. There is usually progressive deterioration, but acute exacerbation may occur. The presence of a thoracic goiter (>50% of the mass below the thoracic inlet) is per se an indication for resection. Tracheal compression by (cervical or thoracic) goiter is also an indication for resection; early tracheal decompression is recommended particularly in symptomatic patients. In severe respiratory distress, intubation and semi-urgent operation may be required. With early intervention, most intrathoracic goiters can be removed through a cervical approach, while tracheomalacia is avoided. We hereby present successful and uncomplicated total thyroidectomy, through a median sternotomy, of a benign, gigantic, bilateral, retrovascular, posterior mediastinal, intrathoracic goiter, encircling the trachea, and causing severe respiratory distress in a 63 year old man with history of previous subtotal thyroidectomy.
Keywords: Airway obstruction/etiology; airway obstruction/surgery; goiter; goiter/intrathoracic; substernal/surgery; thyroidectomy.
Figures


References
-
- Katlic MR, Wang CA, Grillo HC. Substernal goiter. Ann Thorac Surg 1985;39:391-9 - PubMed
-
- Singh B, Lucente FE, Shaha AR. Substernal goiter: a clinical review. Am J Otolaryngol 1994;15:409-16 - PubMed
-
- Netterville JL, Coleman SC, Smith JC, et al. Management of substernal goiter. Laryngoscope 1998;108:1611-7 - PubMed
-
- Hedayati N, McHenry CR. The clinical presentation and operative management of nodular and diffuse substernal thyroid disease. Am Surg 2002;68:245-51; discussion 251-2 - PubMed
-
- Batori M, Chatelou E, Straniero A, et al. Substernal goiters. Eur Rev Med Pharmacol Sci 2005;9:355-9 - PubMed
LinkOut - more resources
Full Text Sources