

Co-administration of rivaroxaban with drugs that share its elimination pathways: pharmacokinetic effects in healthy subjects
- PMID: 23305158
- PMCID: PMC3769672
- DOI: 10.1111/bcp.12075
Co-administration of rivaroxaban with drugs that share its elimination pathways: pharmacokinetic effects in healthy subjects
Abstract
Aims: The anticoagulant rivaroxaban is an oral, direct Factor Xa inhibitor for the management of thromboembolic disorders. Metabolism and excretion involve cytochrome P450 3A4 (CYP3A4) and 2J2 (CYP2J2), CYP-independent mechanisms, and P-glycoprotein (P-gp) and breast cancer resistance protein (Bcrp) (ABCG2).
Methods: The pharmacokinetic effects of substrates or inhibitors of CYP3A4, P-gp and Bcrp (ABCG2) on rivaroxaban were studied in healthy volunteers.
Results: Rivaroxaban did not interact with midazolam (CYP3A4 probe substrate). Exposure to rivaroxaban when co-administered with midazolam was slightly decreased by 11% (95% confidence interval [CI] -28%, 7%) compared with rivaroxaban alone. The following drugs moderately affected rivaroxaban exposure, but not to a clinically relevant extent: erythromycin (moderate CYP3A4/P-gp inhibitor; 34% increase [95% CI 23%, 46%]), clarithromycin (strong CYP3A4/moderate P-gp inhibitor; 54% increase [95% CI 44%, 64%]) and fluconazole (moderate CYP3A4, possible Bcrp [ABCG2] inhibitor; 42% increase [95% CI 29%, 56%]). A significant increase in rivaroxaban exposure was demonstrated with the strong CYP3A4, P-gp/Bcrp (ABCG2) inhibitors (and potential CYP2J2 inhibitors) ketoconazole (158% increase [95% CI 136%, 182%] for a 400 mg once daily dose) and ritonavir (153% increase [95% CI 134%, 174%]).
Conclusions: Results suggest that rivaroxaban may be co-administered with CYP3A4 and/or P-gp substrates/moderate inhibitors, but not with strong combined CYP3A4, P-gp and Bcrp (ABCG2) inhibitors (mainly comprising azole-antimycotics, apart from fluconazole, and HIV protease inhibitors), which are multi-pathway inhibitors of rivaroxaban clearance and elimination.
Keywords: P-glycoprotein; cytochrome P450; drug interactions; healthy subjects; rivaroxaban.
© 2013 Bayer Pharma AG. British Journal of Clinical Pharmacology © 2013 The British Pharmacological Society.
Figures
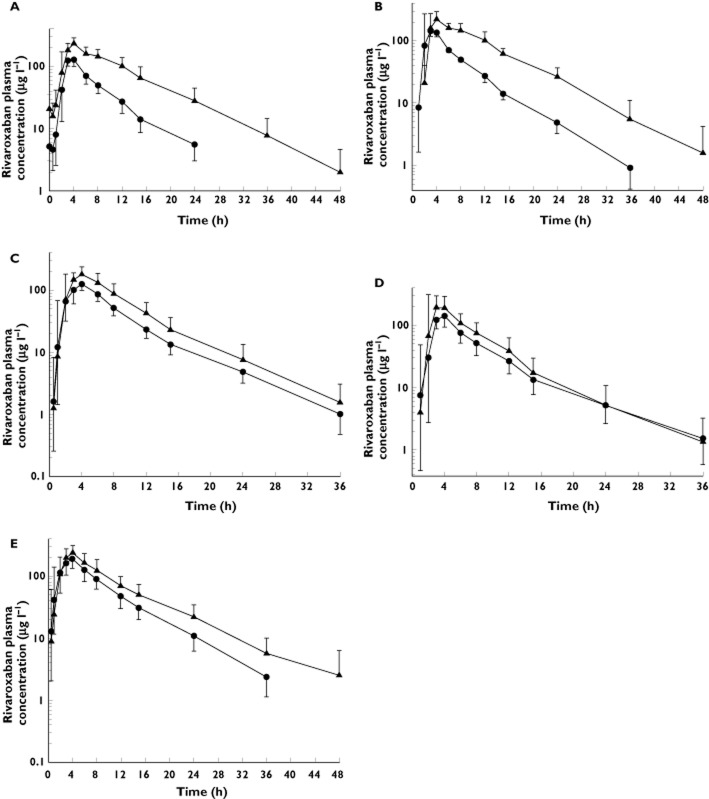
 , rivaroxaban alone (n = 20);
, rivaroxaban alone (n = 20);  , rivaroxaban + ketoconazole (n = 20); (B) steady-state ritonavir (600 mg twice daily for 8 days),
, rivaroxaban + ketoconazole (n = 20); (B) steady-state ritonavir (600 mg twice daily for 8 days),  , rivaroxaban alone (n = 12);
, rivaroxaban alone (n = 12);  , rivaroxaban + ritonavir (n = 12); (C) steady-state clarithromycin (500 mg twice daily for 4 days),
, rivaroxaban + ritonavir (n = 12); (C) steady-state clarithromycin (500 mg twice daily for 4 days),  , rivaroxaban alone (n = 15);
, rivaroxaban alone (n = 15);  , rivaroxaban + clarithromycin (n = 15); (D) steady-state erythromycin (500 mg three times daily for 5 days),
, rivaroxaban + clarithromycin (n = 15); (D) steady-state erythromycin (500 mg three times daily for 5 days),  , rivaroxaban alone (n = 15);
, rivaroxaban alone (n = 15);  , rivaroxaban + erythromycin (n = 15); (E) steady-state fluconazole (400 mg once daily for 6 days),
, rivaroxaban + erythromycin (n = 15); (E) steady-state fluconazole (400 mg once daily for 6 days),  , rivaroxaban alone (n = 13);
, rivaroxaban alone (n = 13);  , rivaroxaban + fluconazole (n = 13)
, rivaroxaban + fluconazole (n = 13)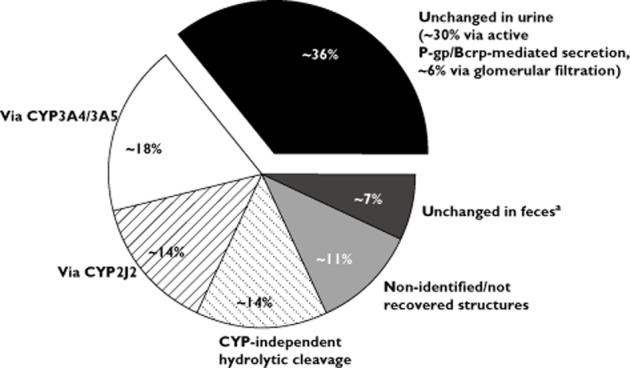
References
-
- Perzborn E, Strassburger J, Wilmen A, Pohlmann J, Roehrig S, Schlemmer KH, Straub A. In vitro and in vivo studies of the novel antithrombotic agent BAY 59-7939 – an oral, direct Factor Xa inhibitor. J Thromb Haemost. 2005;3:514–521. - PubMed
-
- Gerotziafas GT, Elalamy I, Depasse F, Perzborn E, Samama MM. In vitro inhibition of thrombin generation, after tissue factor pathway activation, by the oral, direct Factor Xa inhibitor rivaroxaban. J Thromb Haemost. 2007;5:886–888. - PubMed
-
- Biemond BJ, Perzborn E, Friederich PW, Levi M, Buetehorn U, Büller HR. Prevention and treatment of experimental thrombosis in rabbits with rivaroxaban (BAY 59-7939) – an oral, direct Factor Xa inhibitor. Thromb Haemost. 2007;97:471–477. - PubMed
-
- Perzborn E, Arndt B, Harwardt M, Lange U, Fischer E, Trabant A. Antithrombotic efficacy of BAY 59-7939 – an oral, direct Factor Xa inhibitor – compared with fondaparinux in animal arterial thrombosis and thromboembolic death models. Eur Heart J. 2005;26(Suppl):Abstract P2943.
-
- Turpie AGG, Lassen MR, Eriksson BI, Gent M, Berkowitz SD, Misselwitz F, Bandel TJ, Homering M, Westermeier T, Kakkar AK. Rivaroxaban for the prevention of venous thromboembolism after hip or knee arthroplasty. Pooled analysis of four studies. Thromb Haemost. 2011;105:444–453. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
