

Angiographic features, collaterals, and infarct topography of symptomatic occlusive radiation vasculopathy: a case-referent study
- PMID: 23306321
- PMCID: PMC4156584
- DOI: 10.1161/STROKEAHA.112.674036
Angiographic features, collaterals, and infarct topography of symptomatic occlusive radiation vasculopathy: a case-referent study
Abstract
Background and purpose: Occlusive radiation vasculopathy (ORV) predisposes head-and-neck cancer survivors to ischemic strokes.
Methods: We analyzed the digital subtraction angiography acquired in 96 patients who had first-ever transient ischemic attack or ischemic strokes attributed to ORV. Another age-matched 115 patients who had no radiotherapy but symptomatic high-grade (>70%) carotid stenoses were enrolled as referent subjects. Digital subtraction angiography was performed within 2 months from stroke onset and delineated carotid and vertebrobasilar circulations from aortic arch up to intracranial branches. Two reviewers blinded to group assignment recorded all vascular lesions, collateral status, and infarct pattern.
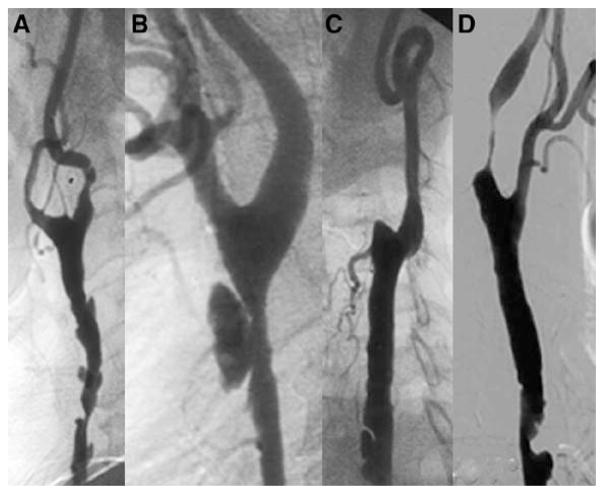
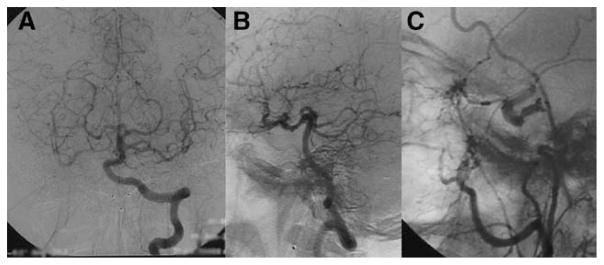
Results: ORV patients had less atherosclerotic risk factors at presentation. In referent patients, high-grade stenoses were mostly focal at the proximal internal carotid artery. In contrast, high-grade ORV lesions diffusely involved the common carotid artery and internal carotid artery and were more frequently bilateral (54% versus 22%), tandem (23% versus 10%), associated with complete occlusion in one or both carotid arteries (30% versus 9%), vertebral artery (VA) steno-occlusions (28% versus 16%), and external carotid artery stenosis (19% versus 5%) (all P<0.05). With comparable rates of vascular anomaly, ORV patients showed more established collateral circulations through leptomeningeal arteries, anterior communicating artery, posterior communicating artery, suboccipital/costocervical artery, and retrograde flow in ophthalmic artery. In terms of infarct topography, the frequencies of cortical or subcortical watershed infarcts were similar in both groups.
Conclusions: ORV angiographic features and corresponding collaterals are distinct from atherosclerotic patterns at initial stroke presentation. Clinical decompensation, despite more extensive collateralization, may precipitate stroke in ORV.
Figures
Similar articles
-
Incomplete circle of Willis is associated with a higher incidence of neurologic events during carotid eversion endarterectomy without shunting.J Vasc Surg. 2018 Dec;68(6):1764-1771. doi: 10.1016/j.jvs.2018.03.429. Epub 2018 Jul 6. J Vasc Surg. 2018. PMID: 29983353
-
Lesion patterns and stroke mechanisms in concurrent atherosclerosis of intracranial and extracranial vessels.Stroke. 2009 Oct;40(10):3211-5. doi: 10.1161/STROKEAHA.109.557041. Epub 2009 Jul 30. Stroke. 2009. PMID: 19644065
-
Angiographically defined collateral circulation and risk of stroke in patients with severe carotid artery stenosis. North American Symptomatic Carotid Endarterectomy Trial (NASCET) Group.Stroke. 2000 Jan;31(1):128-32. doi: 10.1161/01.str.31.1.128. Stroke. 2000. PMID: 10625727 Clinical Trial.
-
Usefulness of transcranial Doppler ultrasound in evaluating cervical-cranial collateral circulations.Interv Neurol. 2013 Oct;2(1):8-18. doi: 10.1159/000354732. Interv Neurol. 2013. PMID: 25187781 Free PMC article. Review.
-
Sequelae and management of radiation vasculopathy in neurosurgical patients.J Neurosurg. 2018 Jun 1;130(6):1889-1897. doi: 10.3171/2017.12.JNS172635. Print 2019 Jun 1. J Neurosurg. 2018. PMID: 29999447 Review.
Cited by
-
Application of Carotid Duplex Ultrasonography in the Surveillance of Carotid Artery Stenosis after Neck Irradiation.Rev Cardiovasc Med. 2022 Jun 27;23(7):240. doi: 10.31083/j.rcm2307240. eCollection 2022 Jul. Rev Cardiovasc Med. 2022. PMID: 39076899 Free PMC article. Review.
-
Total plaque score helps to determine follow-up strategy for carotid artery stenosis progression in head and neck cancer patients after radiation therapy.PLoS One. 2021 Feb 12;16(2):e0246684. doi: 10.1371/journal.pone.0246684. eCollection 2021. PLoS One. 2021. PMID: 33577590 Free PMC article.
-
A Case of Occlusive Radiation Vasculopathy Presenting as Bilateral Internal Carotid Artery, Left Middle Cerebral Artery Occlusion and Literature Review.Case Rep Neurol. 2020 Dec 14;12(Suppl 1):91-96. doi: 10.1159/000501902. eCollection 2020 Sep-Dec. Case Rep Neurol. 2020. PMID: 33505278 Free PMC article.
-
Spotted Temporal Lobe Necrosis following Concurrent Chemoradiation Therapy Using Image-Guided Radiotherapy for Nasopharyngeal Carcinoma.Case Rep Otolaryngol. 2022 Sep 27;2022:5877106. doi: 10.1155/2022/5877106. eCollection 2022. Case Rep Otolaryngol. 2022. PMID: 36204045 Free PMC article.
-
Continuous and Early Progression of Carotid Intima-Media Thickness after Radiotherapy for Head and Neck Cancer: 5-Year Prospective Observational Study.Cerebrovasc Dis. 2023;52(5):543-551. doi: 10.1159/000528622. Epub 2023 Jan 30. Cerebrovasc Dis. 2023. PMID: 36716719 Free PMC article.
References
-
- Plummer C, Henderson RD, O’Sullivan JD, Read SJ. Ischemic stroke and transient ischemic attack after head and neck radiotherapy: a review. Stroke. 2011;42:2410–2418. - PubMed
-
- Haynes JC, Machtay M, Weber RS, Weinstein GS, Chalian AA, Rosenthal DI. Relative risk of stroke in head and neck carcinoma patients treated with external cervical irradiation. Laryngoscope. 2002;112:1883–1887. - PubMed
-
- Dorresteijn LD, Kappelle AC, Boogerd W, Klokman WJ, Balm AJ, Keus RB, et al. Increased risk of ischemic stroke after radiotherapy on the neck in patients younger than 60 years. J Clin Oncol. 2002;20:282–288. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
