

Cough aerosols of Mycobacterium tuberculosis predict new infection: a household contact study
- PMID: 23306539
- PMCID: PMC3707366
- DOI: 10.1164/rccm.201208-1422OC
Cough aerosols of Mycobacterium tuberculosis predict new infection: a household contact study
Abstract
Rationale: Airborne transmission of Mycobacterium tuberculosis results from incompletely characterized host, bacterial, and environmental factors. Sputum smear microscopy is associated with considerable variability in transmission.
Objectives: To evaluate the use of cough-generated aerosols of M. tuberculosis to predict recent transmission.
Methods: Patients with pulmonary tuberculosis (TB) underwent a standard evaluation and collection of cough aerosol cultures of M. tuberculosis. We assessed household contacts for new M. tuberculosis infection. We used multivariable logistic regression analysis with cluster adjustment to analyze predictors of new infection.
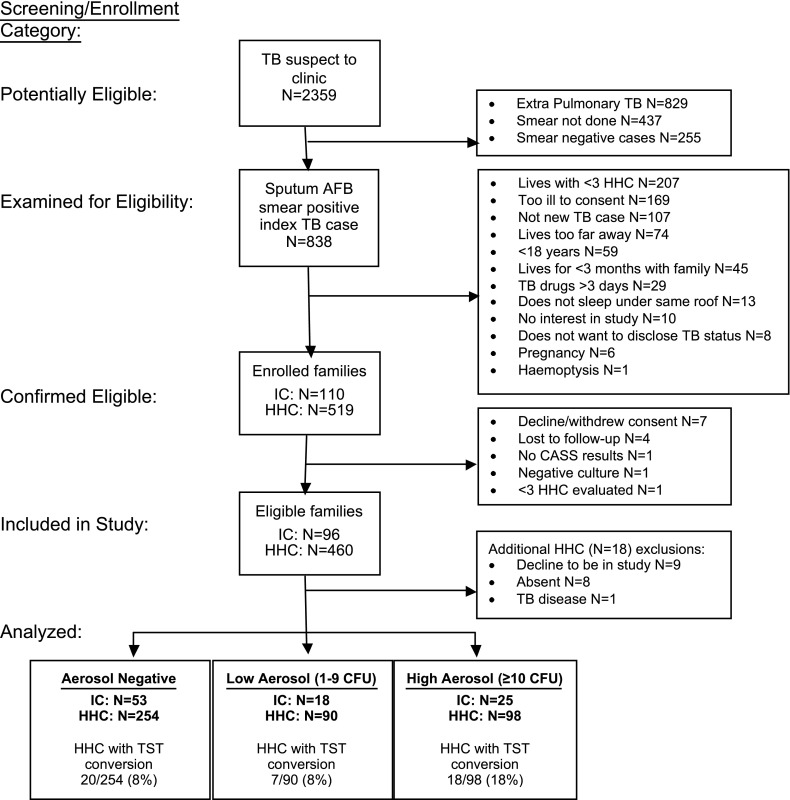
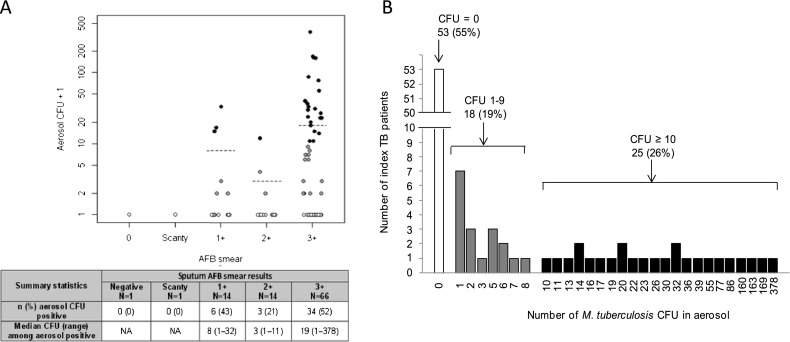
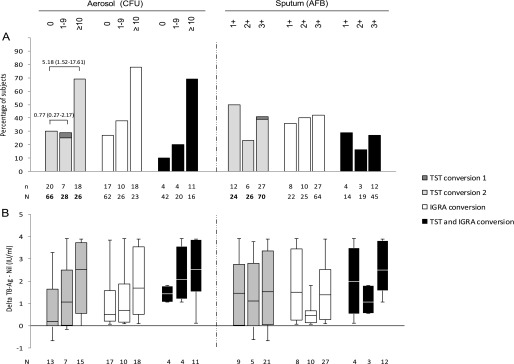
Measurements and main results: From May 2009 to January 2011, we enrolled 96 sputum culture-positive index TB cases and their 442 contacts. Only 43 (45%) patients with TB yielded M. tuberculosis in aerosols. Contacts of patients with TB who produced high aerosols (≥10 CFU) were more likely to have a new infection compared with contacts from low-aerosol (1-9 CFU) and aerosol-negative cases (69%, 25%, and 30%, respectively; P = 0.009). A high-aerosol patient with TB was the only predictor of new M. tuberculosis infection in unadjusted (odds ratio, 5.18; 95% confidence interval, 1.52-17.61) and adjusted analyses (odds ratio, 4.81; 95% confidence interval, 1.20-19.23). Contacts of patients with TB with no aerosols versus low and high aerosols had differential tuberculin skin test and interferon-γ release assay responses.
Conclusions: Cough aerosols of M. tuberculosis are produced by a minority of patients with TB but predict transmission better than sputum smear microscopy or culture. Cough aerosols may help identify the most infectious patients with TB and thus improve the cost-effectiveness of TB control programs.
Figures
References
-
- World Health Organization. Global tuberculosis control: WHO report 2011. Geneva, Switzerland: World Health Organization; 2011. Contract No.: WHO/HTM/TB/2011.16.
-
- Roy CJ, Milton DK. Airborne transmission of communicable infection–the elusive pathway. N Engl J Med. 2004;350:1710–1712. - PubMed
-
- Sultan L, Nyka W, Mills C, O'Grady F, Wells W, Riley RL. Tuberculosis disseminators: a study of the variability of aerial infectivity of tuberculous patients. Am Rev Respir Dis. 1960;82:358–369. - PubMed
-
- Borgdorff M, Nagelkerke NJ, de Haas PE, van Soolingen D. Transmission of Mycobacterium tuberculosis depending on the age and sex of source cases. Am J Epidemiol. 2001;154:934–943. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
