

Clinical risk factors for primary graft dysfunction after lung transplantation
- PMID: 23306540
- PMCID: PMC3733407
- DOI: 10.1164/rccm.201210-1865OC
Clinical risk factors for primary graft dysfunction after lung transplantation
Abstract
Rationale: Primary graft dysfunction (PGD) is the main cause of early morbidity and mortality after lung transplantation. Previous studies have yielded conflicting results for PGD risk factors.
Objectives: We sought to identify donor, recipient, and perioperative risk factors for PGD.
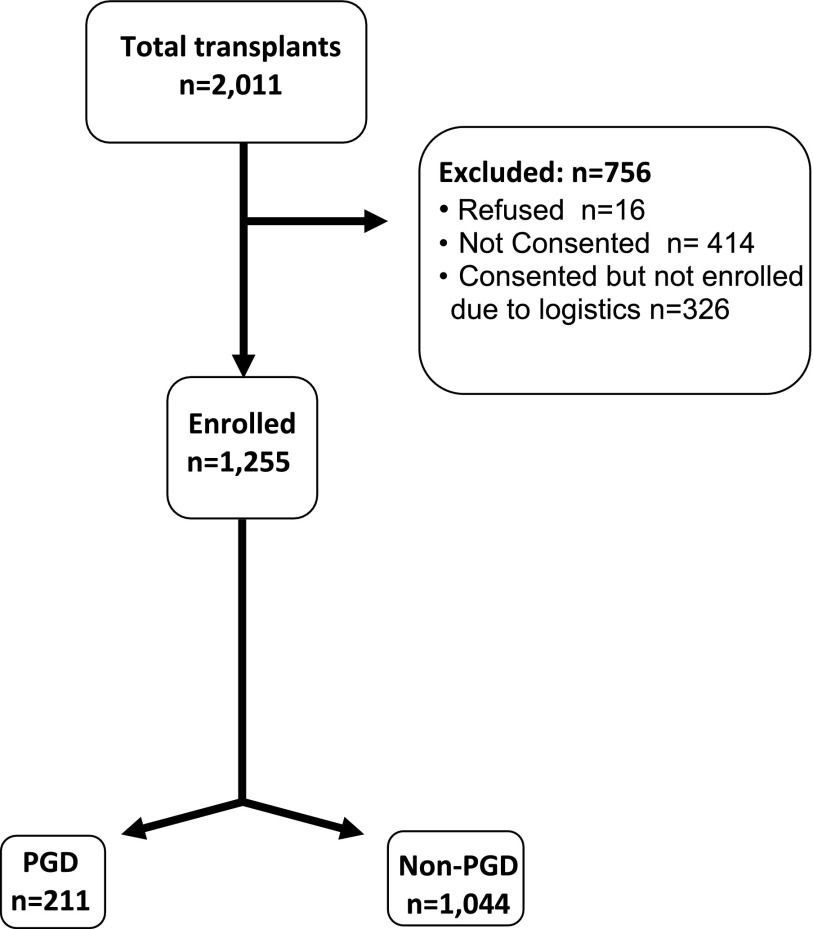
Methods: We performed a 10-center prospective cohort study enrolled between March 2002 and December 2010 (the Lung Transplant Outcomes Group). The primary outcome was International Society for Heart and Lung Transplantation grade 3 PGD at 48 or 72 hours post-transplant. The association of potential risk factors with PGD was analyzed using multivariable conditional logistic regression.
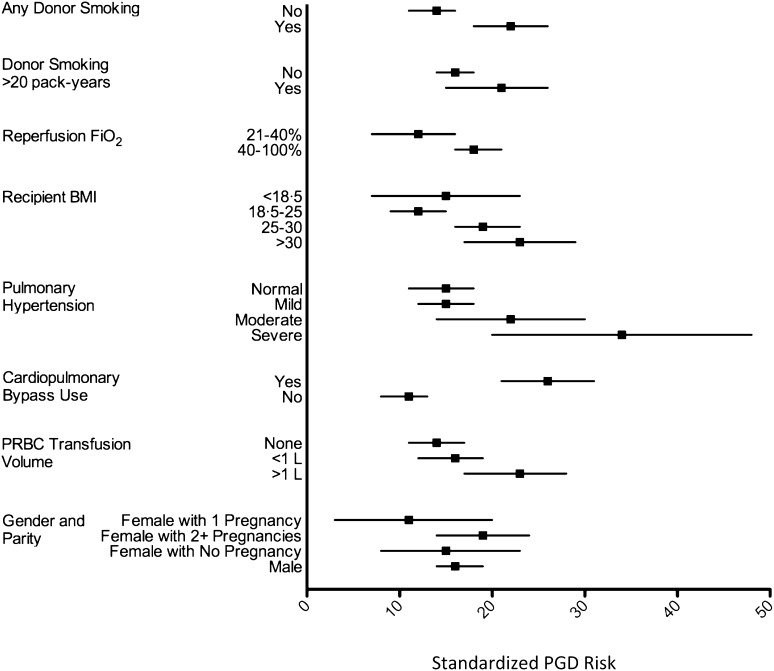
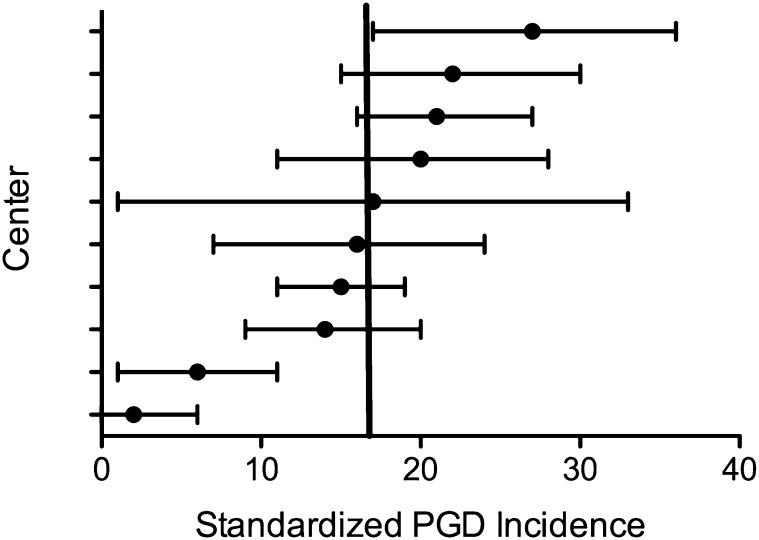
Measurements and main results: A total of 1,255 patients from 10 centers were enrolled; 211 subjects (16.8%) developed grade 3 PGD. In multivariable models, independent risk factors for PGD were any history of donor smoking (odds ratio [OR], 1.8; 95% confidence interval [CI], 1.2-2.6; P = 0.002); FiO2 during allograft reperfusion (OR, 1.1 per 10% increase in FiO2; 95% CI, 1.0-1.2; P = 0.01); single lung transplant (OR, 2; 95% CI, 1.2-3.3; P = 0.008); use of cardiopulmonary bypass (OR, 3.4; 95% CI, 2.2-5.3; P < 0.001); overweight (OR, 1.8; 95% CI, 1.2-2.7; P = 0.01) and obese (OR, 2.3; 95% CI, 1.3-3.9; P = 0.004) recipient body mass index; preoperative sarcoidosis (OR, 2.5; 95% CI, 1.1-5.6; P = 0.03) or pulmonary arterial hypertension (OR, 3.5; 95% CI, 1.6-7.7; P = 0.002); and mean pulmonary artery pressure (OR, 1.3 per 10 mm Hg increase; 95% CI, 1.1-1.5; P < 0.001). PGD was significantly associated with 90-day (relative risk, 4.8; absolute risk increase, 18%; P < 0.001) and 1-year (relative risk, 3; absolute risk increase, 23%; P < 0.001) mortality.
Conclusions: We identified grade 3 PGD risk factors, several of which are potentially modifiable and should be prioritized for future research aimed at preventative strategies. Clinical trial registered with www.clinicaltrials.gov (NCT 00552357).
Trial registration: ClinicalTrials.gov NCT00552357.
Figures
Comment in
-
Why does the transplanted lung sometimes fail to work?Am J Respir Crit Care Med. 2013 Mar 1;187(5):462-4. doi: 10.1164/rccm.201212-2335ED. Am J Respir Crit Care Med. 2013. PMID: 23457364 No abstract available.
References
-
- Christie JD, Sager JS, Kimmel SE, Ahya VN, Gaughan C, Blumenthal NP, Kotloff RM. Impact of primary graft failure on outcomes following lung transplantation. Chest 2005;127:161–165 - PubMed
-
- Daud SA, Yusen RD, Meyers BF, Chakinala MM, Walter MJ, Aloush AA, Patterson GA, Trulock EP, Hachem RR. Impact of immediate primary lung allograft dysfunction on bronchiolitis obliterans syndrome. Am J Respir Crit Care Med 2007;175:507–513 - PubMed
-
- Whitson BA, Prekker ME, Herrington CS, Whelan TP, Radosevich DM, Hertz MI, Dahlberg PS. Primary graft dysfunction and long-term pulmonary function after lung transplantation. J Heart Lung Transplant 2007;26:1004–1011 - PubMed
-
- Barr ML, Kawut SM, Whelan TP, Girgis R, Bottcher H, Sonett J, Vigneswaran W, Follette DM, Corris PA. Report of the ISHLT Working Group on Primary Lung Graft Dysfunction part IV: recipient-related risk factors and markers. J Heart Lung Transplant 2005;24:1468–1482 - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
