

Effects of infection control measures on acquisition of five antimicrobial drug-resistant microorganisms in a tetanus intensive care unit in Vietnam
- PMID: 23306583
- PMCID: PMC3607730
- DOI: 10.1007/s00134-012-2771-1
Effects of infection control measures on acquisition of five antimicrobial drug-resistant microorganisms in a tetanus intensive care unit in Vietnam
Abstract
Purpose: To quantify the effects of barrier precautions and antibiotic mixing on prevalence and acquisition of five drug-resistant microorganisms within a single tetanus intensive care unit at a tertiary referral hospital in Ho Chi Minh City, Vietnam.
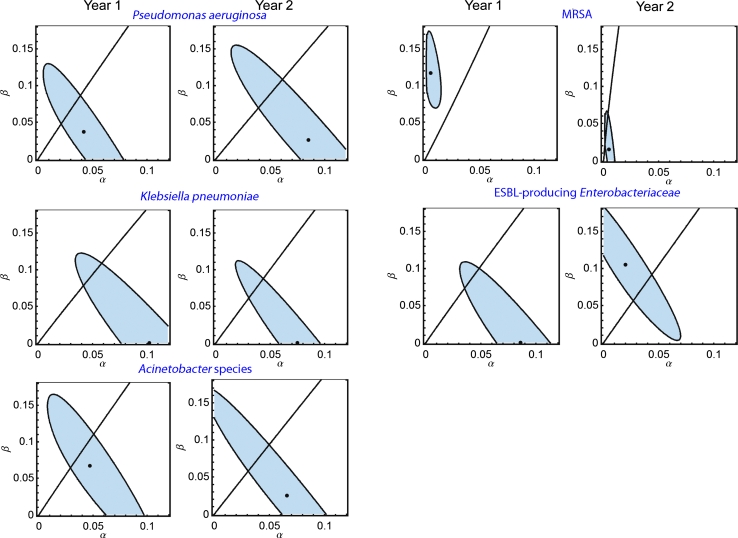
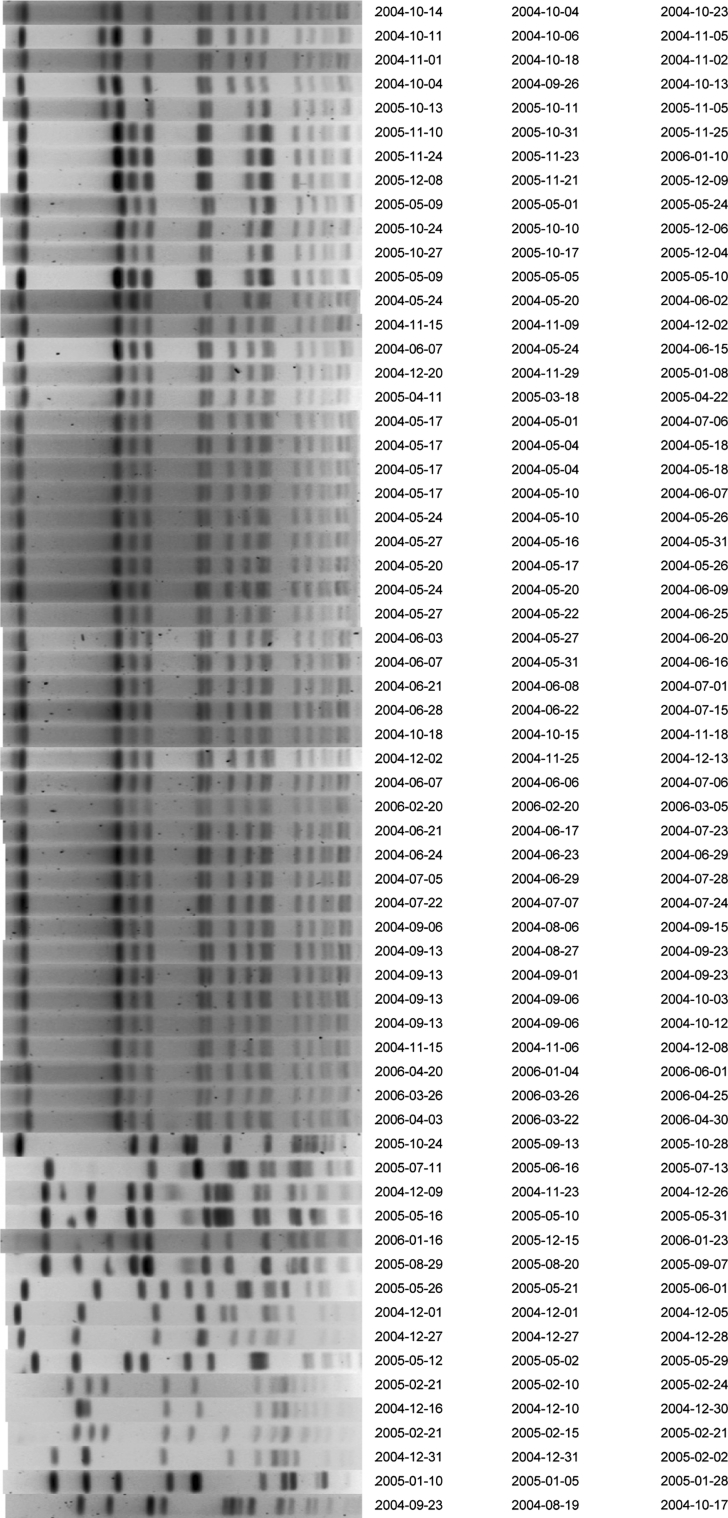
Methods: All patients admitted within the study period were included. After a 1-year baseline period, barrier precautions were implemented and the single empirical treatment ceftazidime was changed to mixing (per consecutive patient) of three different regimens (ceftazidime, ciprofloxacin, piperacillin-tazobactam). Markov chain modeling and genotyping were used to determine the effects of interventions on prevalence levels and the relative importance of cross-transmission and antibiotic-associated selection.
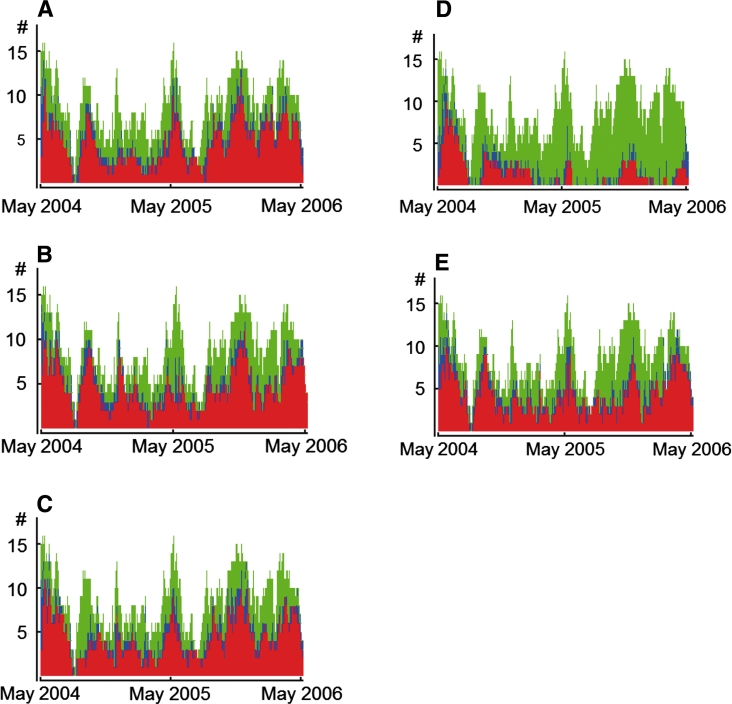
Results: A total of 190 patients were included in year 1 (2,708 patient days, 17,260 cultures) and 167 patients in year 2 (3,384 patient days, 20,580 cultures). In year 1, average daily prevalence rates for methicillin-resistant Staphylococcus aureus (MRSA), extended spectrum beta-lactamase (ESBL)-producing Enterobacteriaceae (excluding Klebsiella pneumoniae), Pseudomonas aeruginosa, gentamicin-resistant K. pneumoniae, and amikacin-resistant Acinetobacter species were 34.0, 61.3, 53.4, 65.7 and 57.1 %. After intervention, ceftazidime usage decreased by 53 %; the use of piperacillin-tazobactam and ciprofloxacin increased 7.2-fold and 4.5-fold, respectively. Adherence to hand hygiene after patient contact was 54 %. These measures were associated with a reduction of MRSA prevalence by 69.8 % (to 10.3 %), mainly because of less cross-transmission (88 % reduction), and of ESBL-producing Enterobacteriaceae prevalence by 10.3 % (non-significantly). In contrast, prevalence levels of the other three pathogens remained unaffected.
Conclusion: The combination of simple infection control measures and antibiotic mixing was highly effective in reducing the prevalence of MRSA, but not of Gram-negative microorganisms.
Figures
References
-
- Rosenthal VD, Maki DG, Salomao R, Moreno CA, Mehta Y, Higuera F, Cuellar LE, Arikan OA, Abouqal R, Leblebicioglu H. Device-associated nosocomial infections in 55 intensive care units of 8 developing countries. Ann Intern Med. 2006;145(8):582–591. - PubMed
-
- Basu S, Andrews JR, Poolman EM, Gandhi NR, Shah NS, Moll A, Moodley P, Galvani AP, Friedland GH. Prevention of nosocomial transmission of extensively drug-resistant tuberculosis in rural South African district hospitals: an epidemiological modelling study. Lancet. 2007;370:1500–1507. doi: 10.1016/S0140-6736(07)61636-5. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
