

Lower tidal volume strategy (≈3 ml/kg) combined with extracorporeal CO2 removal versus 'conventional' protective ventilation (6 ml/kg) in severe ARDS: the prospective randomized Xtravent-study
- PMID: 23306584
- PMCID: PMC3625408
- DOI: 10.1007/s00134-012-2787-6
Lower tidal volume strategy (≈3 ml/kg) combined with extracorporeal CO2 removal versus 'conventional' protective ventilation (6 ml/kg) in severe ARDS: the prospective randomized Xtravent-study
Abstract
Background: Acute respiratory distress syndrome is characterized by damage to the lung caused by various insults, including ventilation itself, and tidal hyperinflation can lead to ventilator induced lung injury (VILI). We investigated the effects of a low tidal volume (V(T)) strategy (V(T) ≈ 3 ml/kg/predicted body weight [PBW]) using pumpless extracorporeal lung assist in established ARDS.
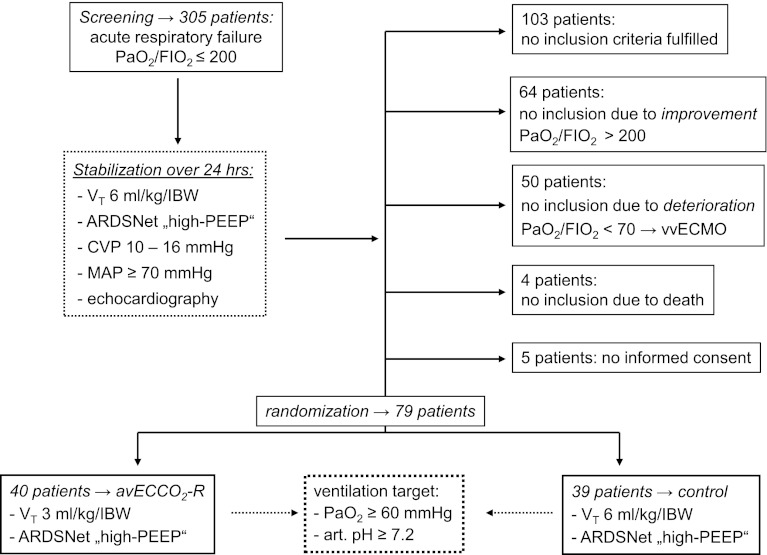
Methods: Seventy-nine patients were enrolled after a 'stabilization period' (24 h with optimized therapy and high PEEP). They were randomly assigned to receive a low V(T) ventilation (≈3 ml/kg) combined with extracorporeal CO2 elimination, or to a ARDSNet strategy (≈6 ml/kg) without the extracorporeal device. The primary outcome was the 28-days and 60-days ventilator-free days (VFD). Secondary outcome parameters were respiratory mechanics, gas exchange, analgesic/sedation use, complications and hospital mortality.
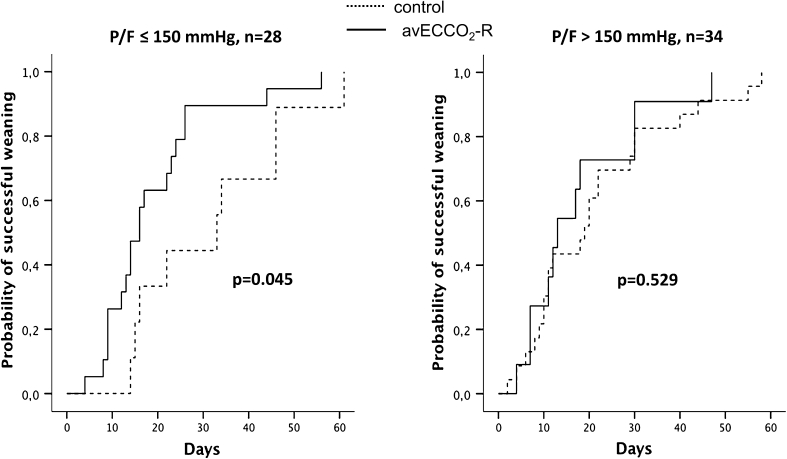
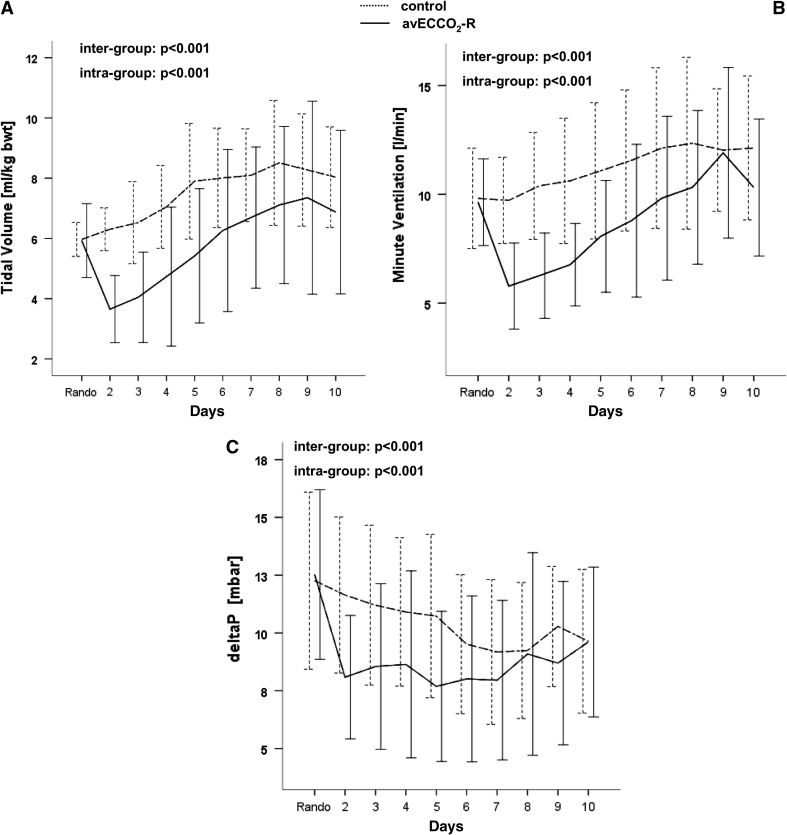
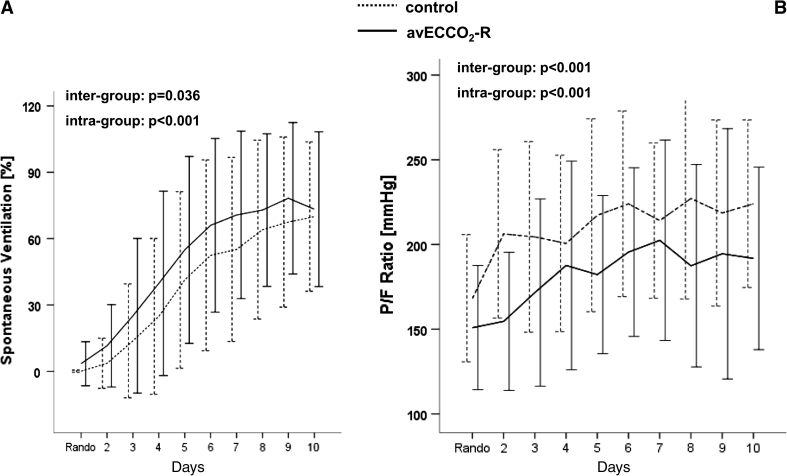
Results: Ventilation with very low V(T)'s was easy to implement with extracorporeal CO2-removal. VFD's within 60 days were not different between the study group (33.2 ± 20) and the control group (29.2 ± 21, p = 0.469), but in more hypoxemic patients (PaO2/FIO2 ≤150) a post hoc analysis demonstrated significant improved VFD-60 in study patients (40.9 ± 12.8) compared to control (28.2 ± 16.4, p = 0.033). The mortality rate was low (16.5%) and did not differ between groups.
Conclusions: The use of very low V(T) combined with extracorporeal CO2 removal has the potential to further reduce VILI compared with a 'normal' lung protective management. Whether this strategy will improve survival in ARDS patients remains to be determined (Clinical trials NCT 00538928).
Trial registration: ClinicalTrials.gov NCT00538928.
Figures
Comment in
-
From protective ventilation to super-protective ventilation for acute respiratory distress syndrome.Intensive Care Med. 2013 May;39(5):963-5. doi: 10.1007/s00134-012-2805-8. Epub 2013 Jan 10. Intensive Care Med. 2013. PMID: 23306587 Free PMC article. No abstract available.
References
-
- Terragni PP, Rosboch G, Tealdi A, Corno E, Menaldo E, Davini O, Gandini G, Herrmann P, Mascia L, Quintel M, Slutsky AS, Gattinoni L, Ranieri VM. Tidal hyperinflation during low tidal volume ventilation in acute respiratory distress syndrome. Am J Respir Crit Care Med. 2007;175:160–166. doi: 10.1164/rccm.200607-915OC. - DOI - PubMed
-
- Grasso S, Stripoli T, Sacchi M, Sacchi M, Trerotoli P, Staffieri F, Franchini D, De Monte V, Valentini V, Pugliese P, Crovace A, Driessen B, Fiore T. Inhomogeneity of lung parenchyma during the open lung strategy: a computed tomography scan study. Am J Respir Crit Care Med. 2009;180:415–423. doi: 10.1164/rccm.200901-0156OC. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
