

Combined endoscopic and laparoscopic surgery may be an alternative to bowel resection for the management of colon polyps not removable by standard colonoscopy
- PMID: 23306590
- PMCID: PMC3657342
- DOI: 10.1007/s00464-012-2714-5
Combined endoscopic and laparoscopic surgery may be an alternative to bowel resection for the management of colon polyps not removable by standard colonoscopy
Abstract
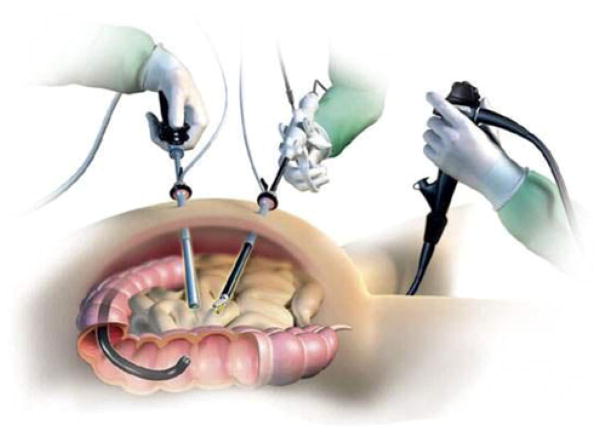
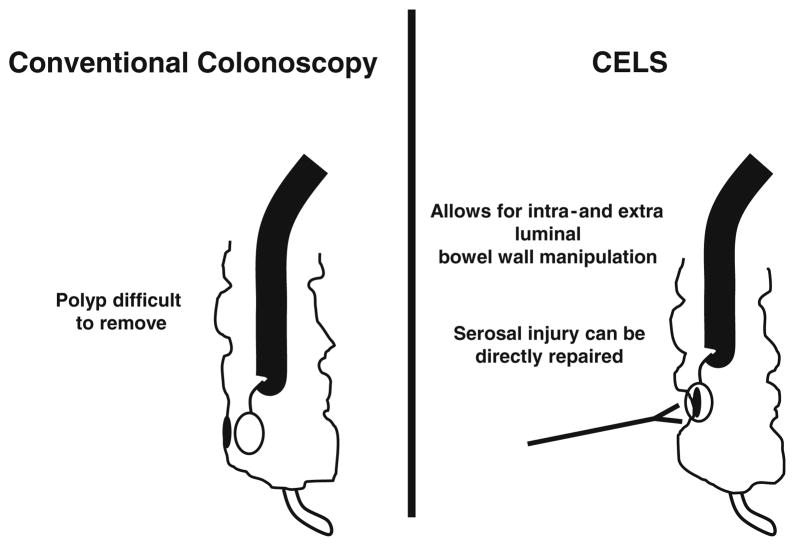
Background: Benign colon polyps may require bowel resection if endoscopic polypectomy cannot be performed to assess adequately for cancer. However, endoscopic removal still may be possible using combined endoscopic and laparoscopic surgery (CELS). The CELS procedure allows for intra- and extraluminal manipulation of the bowel wall to facilitate polyp removal, thereby avoiding bowel resection. This study evaluated the authors' institutional experience with CELS in this patient population.
Methods: Between August 2008 and October 2012, all patients referred to undergo surgery for a benign colon polyp were retrospectively reviewed for operative characteristics, pathology, and postoperative outcomes. Of 14 patients, five were considered candidates for CELS and were compared with nine patients who underwent resection.
Results: The average patient age was similar between the two groups (CELS, 64.9 years vs. resection, 68.3 years). The mean polyp size was 2.3 cm in the CELS group and 2.9 cm in the resection group. In the CELS group, polyps were successfully removed in all cases. The mean operating room time was 159 min in the CELS group and 205 min in the resection group. The median hospital stay was 1 day in the CELS group and 5 days in the resection group. No complications occurred in the CELS group. Two patients in the resection group (22 %) experienced a wound infection. One patient had a postoperative ileus (11 %). Four patients in the CELS group had a benign adenoma. One patient had a benign frozen section evaluation, but the final pathology showed adenocarcinoma requiring a subsequent colectomy. In the resection group, six patients had a benign adenoma, and three patients had a T1N0 cancer. In the CELS group, repeat endoscopy was performed an average of 9.9 months after CELS. Two patients had a residual polyp, and two patients had new polyps in a different location. All were successfully removed.
Conclusion: For benign-appearing polyps not amenable to endoscopic techniques alone, CELS may be an alternative to formal bowel resection for carefully selected patients. The CELS procedure can be performed safely with minimal morbidity and with outcomes that compare favorably with those of formal colectomy.
Conflict of interest statement
Figures
Similar articles
-
Avoiding colorectal resection for polyps: is CELS the best method?Surg Endosc. 2016 Mar;30(3):807-18. doi: 10.1007/s00464-015-4279-6. Epub 2015 Jun 20. Surg Endosc. 2016. PMID: 26092011
-
Combined endoscopic and laparoscopic surgery for the treatment of complex benign colonic polyps (CELS): Observational study.Cir Esp (Engl Ed). 2022 Apr;100(4):215-222. doi: 10.1016/j.cireng.2022.03.005. Epub 2022 Apr 14. Cir Esp (Engl Ed). 2022. PMID: 35431169
-
Combined endo-laparoscopic surgery (CELS) for benign colon polyps: a single institution cost analysis.Surg Endosc. 2019 Oct;33(10):3238-3242. doi: 10.1007/s00464-018-06610-z. Epub 2018 Dec 3. Surg Endosc. 2019. PMID: 30511309
-
Combined endoscopic-laparoscopic surgery (CELS) can avoid segmental colectomy in endoscopically unremovable colonic polyps: a cohort study over 10 years.Surg Endosc. 2022 Jan;36(1):196-205. doi: 10.1007/s00464-020-08255-3. Epub 2021 Jan 13. Surg Endosc. 2022. PMID: 33439344
-
[Combined endoscopic laparoscopic colon polypectomy].Ugeskr Laeger. 2017 Apr 10;179(15):V11160803. Ugeskr Laeger. 2017. PMID: 28416054 Review. Danish.
Cited by
-
Combined Endoscopic Laparoscopic Surgery Procedures for Colorectal Surgery.Clin Colon Rectal Surg. 2017 Apr;30(2):145-150. doi: 10.1055/s-0036-1597321. Clin Colon Rectal Surg. 2017. PMID: 28381946 Free PMC article. Review.
-
Multimodality Imaging Review of Anorectal and Perirectal Diseases With Histological, Endoscopic, and Operative Correlation, Part I: Anatomy and Neoplasms.Curr Probl Diagn Radiol. 2019 Sep-Oct;48(5):494-508. doi: 10.1067/j.cpradiol.2018.07.015. Epub 2018 Jul 29. Curr Probl Diagn Radiol. 2019. PMID: 30172447 Free PMC article. Review.
-
Combined endo-laparoscopic surgery for difficult benign colorectal polyps.J Gastrointest Oncol. 2020 Jun;11(3):475-485. doi: 10.21037/jgo.2019.12.11. J Gastrointest Oncol. 2020. PMID: 32655925 Free PMC article. Review.
-
Hybrid surgery for early gastric cancer.Transl Gastroenterol Hepatol. 2016 Apr 6;1:26. doi: 10.21037/tgh.2016.03.23. eCollection 2016. Transl Gastroenterol Hepatol. 2016. PMID: 28138593 Free PMC article. Review.
-
Management of complex polyps of the colon and rectum.Int J Colorectal Dis. 2018 Feb;33(2):115-129. doi: 10.1007/s00384-017-2950-1. Epub 2017 Dec 28. Int J Colorectal Dis. 2018. PMID: 29282496 Review.
References
-
- Jang JH, Balik E, Kirchoff D, Tromp W, Kumar A, Grieco M, Feingold DL, Cekic V, Njoh L, Whelan RL. Oncologic colorectal resection, not advanced endoscopic polypectomy, is the best treatment for large dysplastic adenomas. J Gastrointest Surg. 2012;16:165–171. Discussion 171–162. - PubMed
-
- Yan J, Trencheva K, Lee SW, Sonoda T, Shukla P, Milsom JW. Treatment for right colon polyps not removable using standard colonoscopy: combined laparoscopic–colonoscopic approach. Dis Colon Rectum. 2011;54:753–758. - PubMed
-
- Whelan RL. Laparoscopic-facilitated colonic endoscopic mucosal resection and endoscopic submucosal resection of adenomas: techniques to avoid segmental colectomy. J Gastrointest Surg. 2011;15:1309–1312. - PubMed
-
- Nakajima K, Lee SW, Sonoda T, Milsom JW. Intraoperative carbon dioxide colonoscopy: a safe insufflation alternative for locating colonic lesions during laparoscopic surgery. Surg Endosc. 2005;19:321–325. - PubMed
-
- Zmora O, Dinnewitzer AJ, Pikarsky AJ, Efron JE, Weiss EG, Nogueras JJ, Wexner SD. Intraoperative endoscopy in laparoscopic colectomy. Surg Endosc. 2002;16:808–811. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
