

Rotator cuff tear: physical examination and conservative treatment
- PMID: 23306597
- PMCID: PMC3607722
- DOI: 10.1007/s00776-012-0345-2
Rotator cuff tear: physical examination and conservative treatment
Abstract
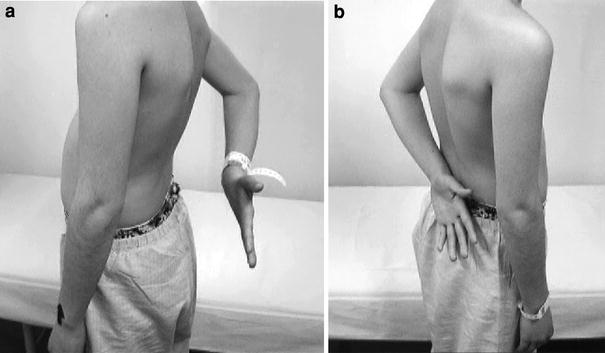
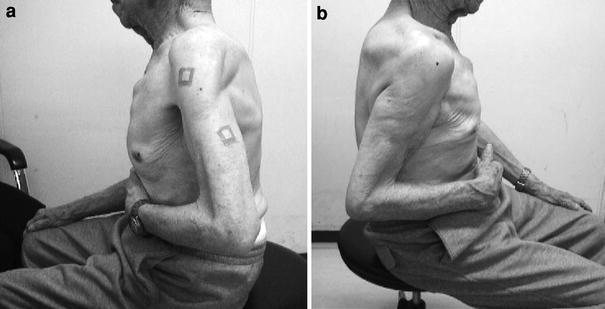
Rotator cuff tear is one of the most common shoulder diseases. It is interesting that some rotator cuff tears are symptomatic, whereas others are asymptomatic. Pain is the most common symptom of patients with a tear. Even in patients with an asymptomatic tear, it may become symptomatic with an increase in tear size. Physical examination is extremely important to evaluate the presence, location, and extent of a tear. It also helps us to understand the mechanism of pain. Conservative treatment often works. Patients with well-preserved function of the supraspinatus and infraspinatus are the best candidates for conservative treatment. After a successful conservative treatment, the symptom once disappeared may come back again. This recurrence of symptoms is related to tear expansion. Those with high risk of tear expansion and those with less functional rotator cuff muscles are less likely to respond to conservative treatment. They may need a surgical treatment.
Figures







References
-
- Minagawa H, Itoi E, Abe H, Fukuta M, Yamamoto N, Seki N, Kikuchi K. Epidemiology of rotator cuff tears. J Jpn Orthop Assoc. 2006;80:S217 (in Japanese).
-
- Kobayashi M, Itoi E, Minagawa H, Yamamoto N, Tuoheti Y, Saito H, Seki N, Aizawa T, Abe H. Prevalence of the shoulder pain in the middle-aged and the elderly and their choices for the treatment. Katakansetsu 2004;29:179 (in Japanese).
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
