

Desmoplastic small round cell tumour: the radiological, pathological and clinical features
- PMID: 23307783
- PMCID: PMC3579986
- DOI: 10.1007/s13244-012-0212-x
Desmoplastic small round cell tumour: the radiological, pathological and clinical features
Abstract
Objectives: Desmoplastic small round cell tumours (DSRCTs) are rare aggressive tumours of young adults that present late and have poor prognosis. This review discusses distinctive radiological features, histopathology and clinical course of this soft-tissue sarcoma.
Methods: From 1991 to 2012, the radiology of 20 patients with pathologically proven DSRCT was independently reviewed by two experienced radiologists. The clinical presentation, treatment and outcome were recorded.
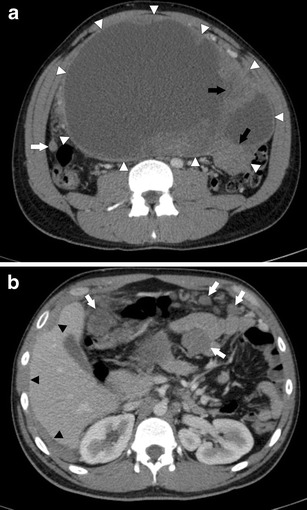
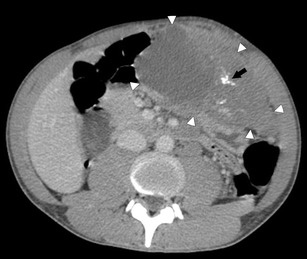
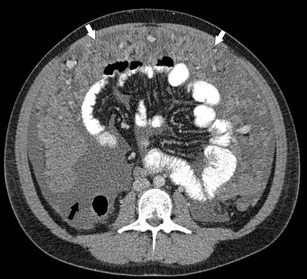
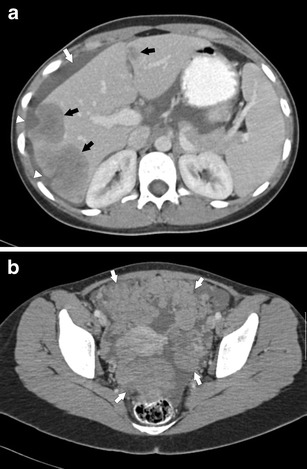
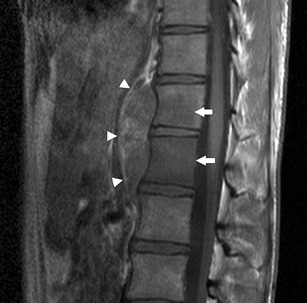
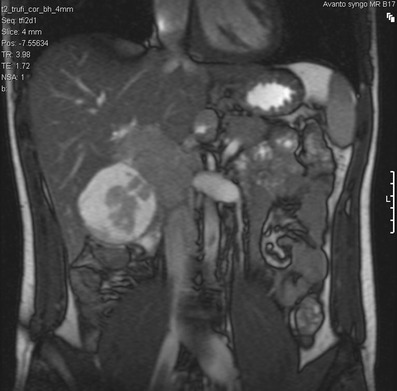
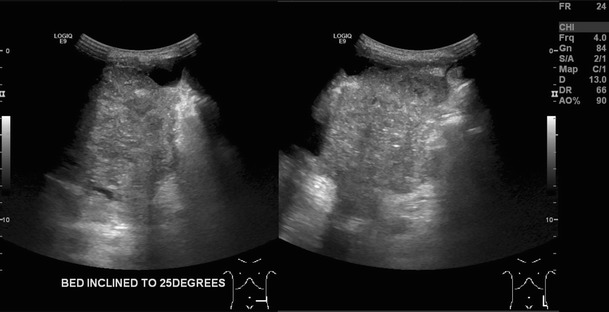
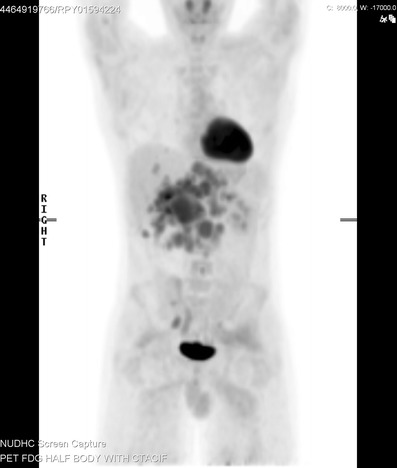
Patients: 16 men, four women; mean age 28.3 years. Computed tomography (CT) demonstrated peritoneal/omental masses without an organ of origin (94 %), with the majority of cases demonstrating large (>5 cm) dominant soft-tissue deposit (80 %) with multiple smaller foci. CT and magnetic resonance imaging (MRI) typically demonstrated heterogeneous soft-tissue enhancement with cystic degeneration. A minority (20 %) demonstrated calcification. Lymph node enlargement occurred in 50 % of cases. Distant metastatic disease occurred in 25 %. Painful abdominal masses were clinically predominant. Treatment strategies include combination chemotherapy with debulking surgery and/or radiotherapy. Median survival from diagnosis was 22.8 months.
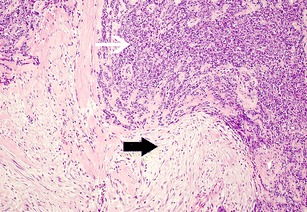
Conclusion: Features of multifocal peritoneal/omental masses, usually in combination with a dominant soft tissue deposit, are distinctive in this rare sarcoma. CT/MRI defines the extent of disease and characterises supporting imaging findings. Prolific desmoplastic reaction histologically separates DSRCT from similar subtypes. Combination treatment strategies can infer a survival benefit but prognosis remains poor. TEACHING POINTS : • DSRCTs are rare tumours of young adults (mean age 28.3 years) with a male predominance (4:1). • Painful abdominal masses clinically predominate. Non-specific features of malignancy can be present. • Multifocal peritoneal masses with a dominant soft tissue lesion is a distinctive imaging finding. • A large desmoplastic reaction differentiates DSRCTs from histologically similar round cell subtypes. • Despite debulking surgery with adjuvant chemotherapy, median survival from diagnosis is 22.3 months.
Figures
References
-
- Gerald WL, Rosai J. Case 2. Desmoplastic small cell tumor with divergent differentiation Pediatr Pathol. 1989;9(2):177–183. - PubMed
-
- Kushner BH, LaQuaglia MP, Wollner N, Meyers PA, Lindsley KL, Ghavimi F, et al. Desmoplastic small round-cell tumor: prolonged progression-free survival with aggressive multimodality therapy. J Clin Oncol. 1996;14(5):1526–1531. - PubMed
-
- Yachnis AT, Rorke LB, Biegel JA, Perilongo G, Zimmerman RA, Sutton LN. Desmoplastic primitive neuroectodermal tumor with divergent differentiation. Broadening the spectrum of desmoplastic infantile neuroepithelial tumors Am J Surg Pathol. 1992;16(10):998–1006. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
