

Comparing mortality of peritoneal and hemodialysis patients in the first 2 years of dialysis therapy: a marginal structural model analysis
- PMID: 23307879
- PMCID: PMC3613949
- DOI: 10.2215/CJN.04810512
Comparing mortality of peritoneal and hemodialysis patients in the first 2 years of dialysis therapy: a marginal structural model analysis
Abstract
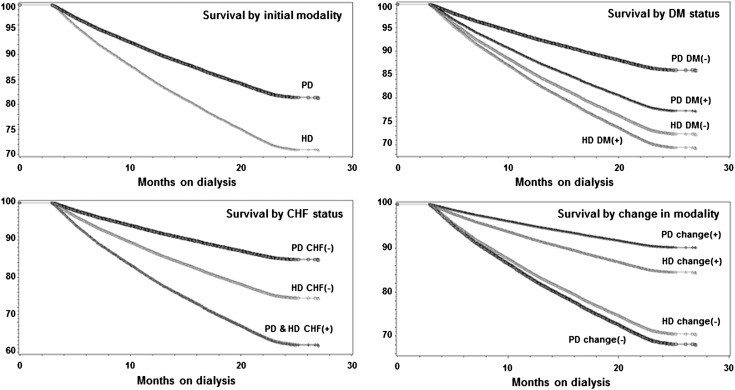
Background and objectives: There are conflicting research results about the survival differences between hemodialysis and peritoneal dialysis, especially during the first 2 years of dialysis treatment. Given the challenges of conducting randomized trials, differential rates of modality switch and transplantation, and time-varying confounding in cohort data during the first years of dialysis treatment, use of novel analytical techniques in observational cohorts can help examine the peritoneal dialysis versus hemodialysis survival discrepancy.
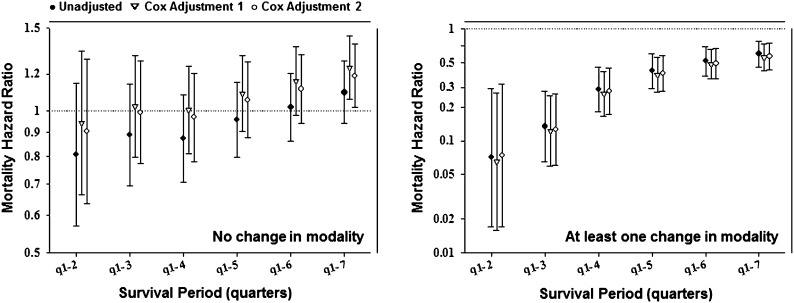
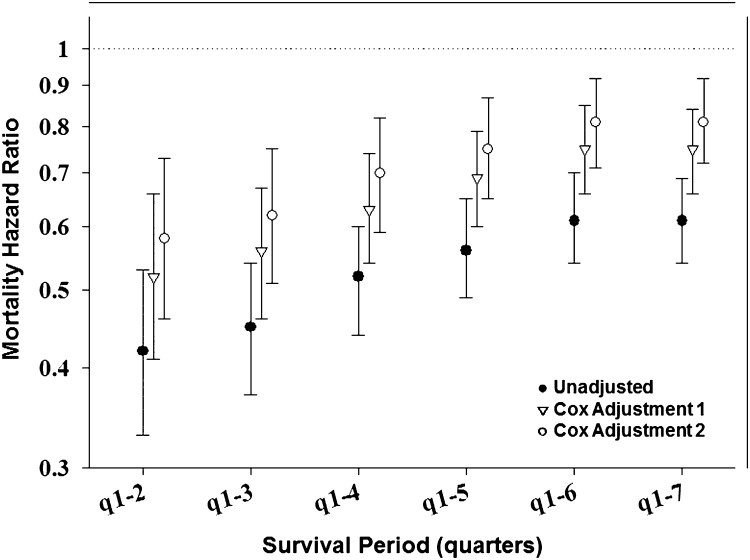
Design, setting, participants, & measurements: This study examined a cohort of incident dialysis patients who initiated dialysis in DaVita dialysis facilities between July of 2001 and June of 2004 and were followed for 24 months. This study used the causal modeling technique of marginal structural models to examine the survival differences between peritoneal dialysis and hemodialysis over the first 24 months, accounting for modality change, differential transplantation rates, and detailed time-varying laboratory measurements.
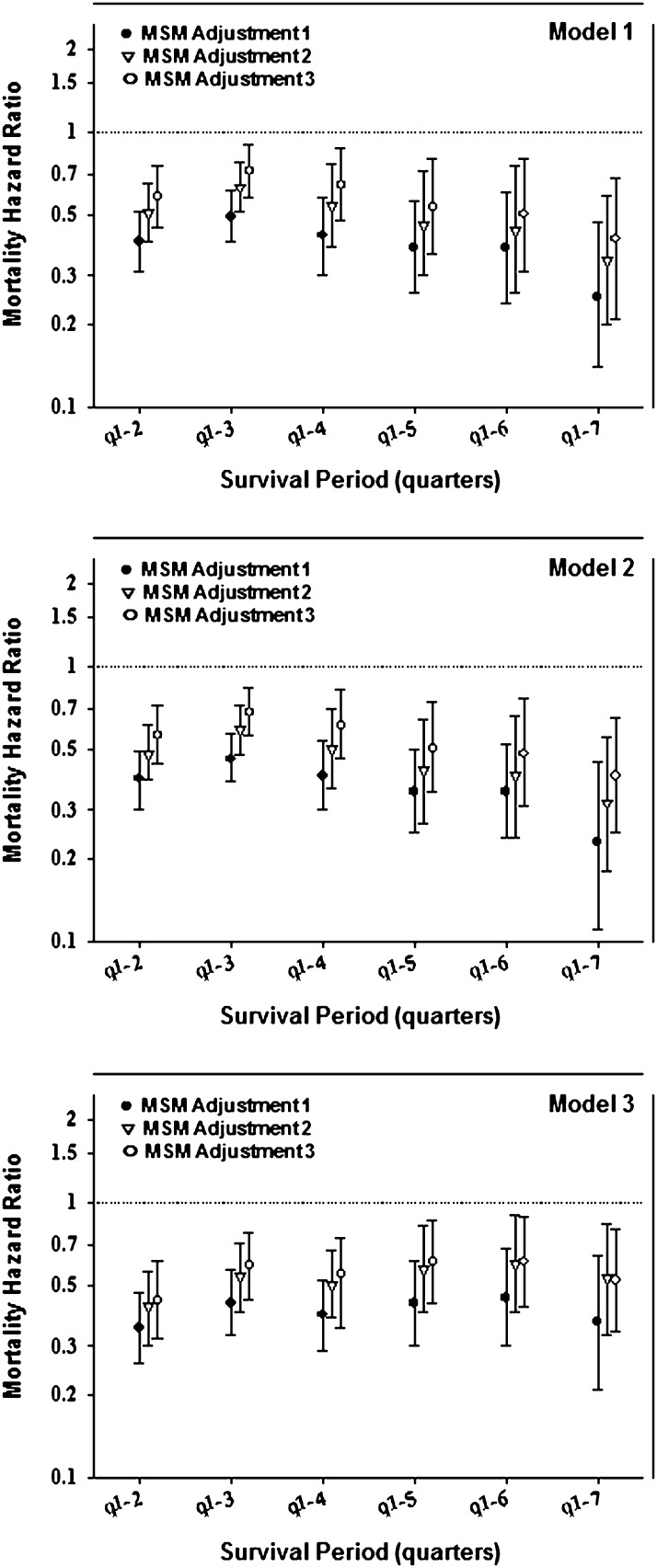
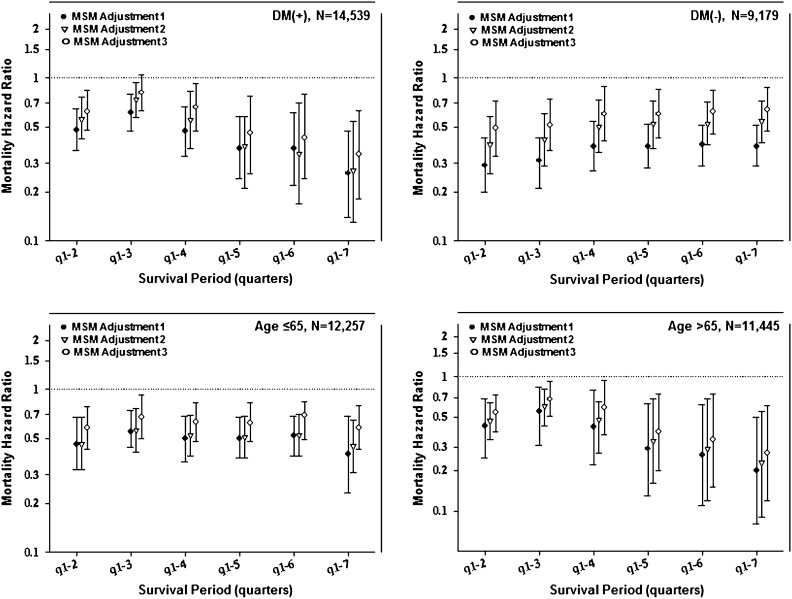
Results: On dialysis treatment day 90, there were 23,718 incident dialysis-22,360 hemodialysis and 1,358 peritoneal dialysis-patients. Incident peritoneal dialysis patients were younger, had fewer comorbidities, and were nine and three times more likely to switch dialysis modality and receive kidney transplantation over the 2-year period, respectively, compared with hemodialysis patients. In marginal structural models analyses, peritoneal dialysis was associated with persistently greater survival independent of the known confounders, including dialysis modality switch and transplant censorship (i.e., death hazard ratio of 0.52 [95% confidence limit 0.34-0.80]).
Conclusions: Peritoneal dialysis seems to be associated with 48% lower mortality than hemodialysis over the first 2 years of dialysis therapy independent of modality switches or differential transplantation rates.
Figures
Comment in
-
Assessments of causal effects--theoretically sound, practically unattainable, and clinically not so relevant.Clin J Am Soc Nephrol. 2013 Apr;8(4):520-2. doi: 10.2215/CJN.02200213. Epub 2013 Mar 21. Clin J Am Soc Nephrol. 2013. PMID: 23520043 No abstract available.
References
-
- US Renal Data System : USRDS 2009 Annual Data Report: Atlas of Chronic Kidney Disease and End-Stage Renal Disease in the United States National Institute of Health Volume 1, Bethesda, MD, National Institute of Health, National Institute of Diabetes and Digestive and Kidney Disease, 2009
-
- US Renal Data System : USRDS 2009 Annual Data Report: Atlas of Chronic Kidney Disease and End-Stage Renal Disease in the United States National Institute of Health Volume 2, Bethesda, MD, National Institute of Health, National Institute of Diabetes and Digestive and Kidney Disease, 2009
-
- Nesrallah G, Mendelssohn DC: Modality options for renal replacement therapy: The integrated care concept revisited. Hemodial Int 10: 143–151, 2006 - PubMed
-
- US Renal Data System : USRDS 2011 Annual Data Report: Atlas of Chronic Kidney Disease and End-Stage Renal Disease in the United States, Bethesda, MD, National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, 2011
-
- Burkart J: The future of peritoneal dialysis in the United States: Optimizing its use. Clin J Am Soc Nephrol 4[Suppl 1]: S125–S131, 2009 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
