

Early experiences and in-hospital results with a novel off-pump apico-aortic conduit
- PMID: 23307931
- PMCID: PMC3598027
- DOI: 10.1093/icvts/ivs513
Early experiences and in-hospital results with a novel off-pump apico-aortic conduit
Abstract
Objectives: To offer surgical treatment in patients with aortic valve stenosis and contraindications for aortic valve replacement (e.g. ostial encroachment and previous mitral valve replacement). The aim of this study was to prove the feasibility and efficacy of this novel innovative off-pump apico-aortic conduit technique.
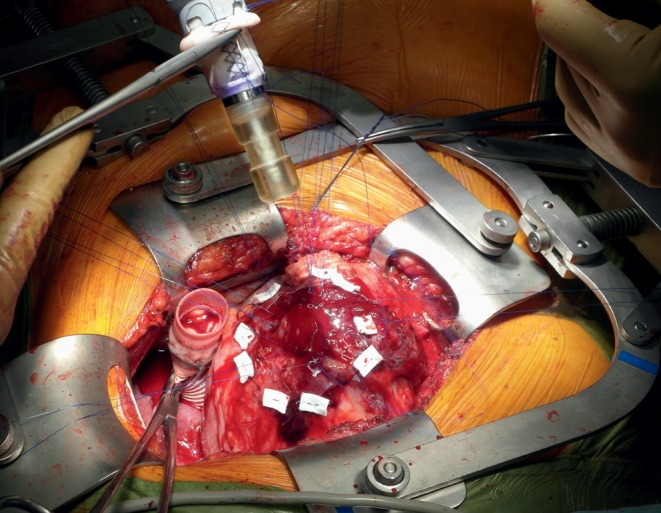
Methods: The bipartite conduit consists of an 18-mm prosthetic tube graft containing a stentless porcine aortic valve as well as a flexible semi-rigid and curved ventricular connector. Via left anterior lateral thoracotomy, the valved conduit is sutured to the descending aorta. The left ventricular connector is implanted with a gun-like applicator into the apex without cardiopulmonary bypass and with minimal blood loss.
Results: Between March and December 2011, 7 patients (5 females/2 males) with a mean age of 82 (79-89 years) were operated on. The mean logistic EuroSCORE I was 36.4 ± 23.7 (median 36.7%). The mean ejection fraction was 37 (25-65%) and the mean preoperative transaortic gradient was 38 (22-53 mmHg). Three patients had previous mechanical mitral valve replacement, 1 had a porcelain aorta and 3 had unfavourable distances between the aortic annulus and ostia (ostial encroachment). Implantation was uneventful in all patients, with need for limited cardiopulmonary bypass in only 1 patient. Postoperative mean transaortic gradient was 14 (11-25 mmHg). Approximately 70% of stroke volume was bypassed as measured in postoperative magnetic resonance. One patient died in hospital due to respiratory failure. New York Heart Association class in the other patients diminished from 3.6 to 1.6. No rhythmic disturbances or heart block were encountered.
Conclusions: With this novel conduit, we observed excellent haemodynamic results. We feel that this additional surgical approach to aortic stenosis in elderly, high-risk patients can augment conventional on-pump and interventional treatments of aortic stenosis.
Figures


Similar articles
-
Aortic valve bypass: experience from Denmark.Interact Cardiovasc Thorac Surg. 2013 Jul;17(1):79-83. doi: 10.1093/icvts/ivt087. Epub 2013 Mar 25. Interact Cardiovasc Thorac Surg. 2013. PMID: 23529752 Free PMC article.
-
Apico-aortic conduit for aortic stenosis with a porcelain aorta; technical modification for apical outflow.Interact Cardiovasc Thorac Surg. 2009 Oct;9(4):703-5. doi: 10.1510/icvts.2009.213959. Epub 2009 Jul 7. Interact Cardiovasc Thorac Surg. 2009. PMID: 19584069
-
Long-term results after aortic root replacement using self-assembled valve composite grafts in patients with small aortic annulus.Interact Cardiovasc Thorac Surg. 2014 Feb;18(2):159-63. doi: 10.1093/icvts/ivt447. Epub 2013 Oct 30. Interact Cardiovasc Thorac Surg. 2014. PMID: 24179177 Free PMC article.
-
Transcatheter aortic valve implantation: anesthetic considerations.Anesth Analg. 2009 May;108(5):1453-62. doi: 10.1213/ane.0b013e31819b07ce. Anesth Analg. 2009. PMID: 19372319 Review.
-
Sutureless Perceval Aortic Valve Versus Conventional Stented Bioprostheses: Meta-Analysis of Postoperative and Midterm Results in Isolated Aortic Valve Replacement.J Am Heart Assoc. 2018 Feb 16;7(4):e006091. doi: 10.1161/JAHA.117.006091. J Am Heart Assoc. 2018. PMID: 29453309 Free PMC article.
Cited by
-
Hemodynamic changes following aortic valve bypass: a mathematical approach.PLoS One. 2015 Apr 16;10(4):e0123000. doi: 10.1371/journal.pone.0123000. eCollection 2015. PLoS One. 2015. PMID: 25881082 Free PMC article.
References
-
- European Commission. Demography report 2010–older, more numerous and diverse Europeans. Eurostat 2011 [accessed 23 October 2012]. Available from: http://ec.europa.eu/social/BlobServlet?docId=6824&langId=en .
-
- Asimakopoulos G, Edwards MB, Taylor KM. Aortic valve replacement in patients 80 years of age and older: survival and cause of death based on 1100 cases: collective results from the UK Heart Valve Registry. Circulation. 1997;96:3403–8. - PubMed
-
- Varadarajan P, Kapoor N, Bansal RC, Pai RG. Clinical profile and natural history of 453 nonsurgically managed patients with severe aortic stenosis. Ann Thorac Surg. 2006;82:2111–5. - PubMed
-
- Cribier A, Eltchaninoff H, Tron C. First human transcatheter implantation of an aortic prosthesis in a case of severe calcific aortic stenosis. Ann Cardiol Angiol (Paris) 2003;52:173–5. - PubMed
-
- Smith CR, Leon MB, Mack MJ, Miller DC, Moses JW, Svensson LG, et al. Transcatheter versus surgical aortic-valve replacement in high-risk patients. N Engl J Med. 2011;364:2187–98. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
