

The use of propofol as a sedative agent in gastrointestinal endoscopy: a meta-analysis
- PMID: 23308191
- PMCID: PMC3540096
- DOI: 10.1371/journal.pone.0053311
The use of propofol as a sedative agent in gastrointestinal endoscopy: a meta-analysis
Abstract
Objectives: To assess the efficacy and safety of propofol sedation for gastrointestinal endoscopy, we conducted a meta-analysis of randomized controlled trials (RCTs) comparing propofol with traditional sedative agents.
Methods: RCTs comparing the effects of propofol and traditional sedative agents during gastrointestinal endoscopy were found on MEDLINE, the Cochrane Central Register of Controlled Trials, and EMBASE. Cardiopulmonary complications (i.e., hypoxia, hypotension, arrhythmia, and apnea) and sedation profiles were assessed.
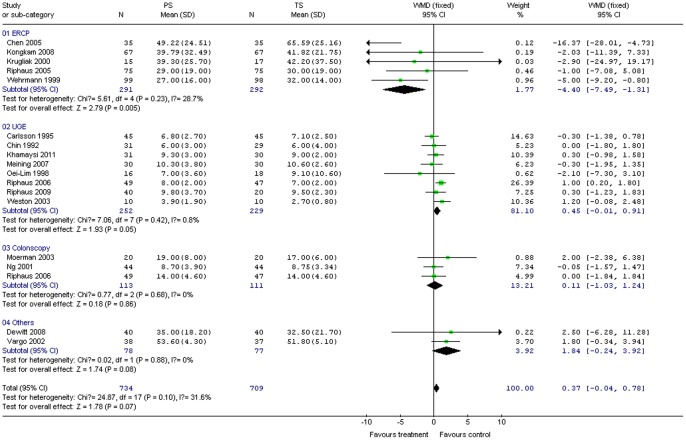
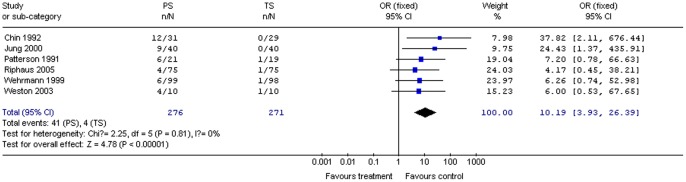
Results: Twenty-two original RCTs investigating a total of 1,798 patients, of whom 912 received propofol only and 886 received traditional sedative agents only, met the inclusion criteria. Propofol use was associated with shorter recovery (13 studies, 1,165 patients; WMD -19.75; 95% CI -27.65, 11.86) and discharge times (seven studies, 471 patients; WMD -29.48; 95% CI -44.13, -14.83), higher post-anesthesia recovery scores (four studies, 503 patients; WMD 2.03; 95% CI 1.59, 2.46), better sedation (nine studies, 592 patients; OR 4.78; 95% CI 2.56, 8.93), and greater patient cooperation (six studies, 709 patients; WMD 1.27; 95% CI 0.53, 2.02), as well as more local pain on injection (six studies, 547 patients; OR 10.19; 95% CI 3.93, 26.39). Effects of propofol on cardiopulmonary complications, procedure duration, amnesia, pain during endoscopy, and patient satisfaction were not found to be significantly different from those of traditional sedative agents.
Conclusions: Propofol is safe and effective for gastrointestinal endoscopy procedures and is associated with shorter recovery and discharge periods, higher post-anesthesia recovery scores, better sedation, and greater patient cooperation than traditional sedation, without an increase in cardiopulmonary complications. Care should be taken when extrapolating our results to specific practice settings and high-risk patient subgroups.
Conflict of interest statement
Figures











References
-
- Cohen LB, Wecsler JS, Gaetano JN, Benson AA, Miller KM, et al. (2006) Endoscopic sedation in the United States: results from a nationwide survey. Am J Gastroenterol 101: 967–974. - PubMed
-
- Ellett ML (2010) A literature review of the safety and efficacy of using propofol for sedation in endoscopy. Gastroenterol Nurs 33: 111–117. - PubMed
-
- Vargo JJ, Zuccaro G Jr, Dumot JA, Shermock KM, Morrow JB, et al. (2002) Gastroenterologist-administered propofol versus meperidine and midazolam for advanced upper endoscopy: a prospective, randomized trial. Gastroenterology 123: 8–16. - PubMed
-
- Amornyotin S, Srikureja W, Chalayonnavin W, Kongphlay S (2011) Dose requirement and complications of diluted and undiluted propofol for deep sedation in endoscopic retrograde cholangiopancreatography. Hepatobiliary Pancreat Dis Int 10: 313–318. - PubMed
-
- Paspatis GA, Chainaki I, Manolaraki MM, Vardas E, Theodoropoulou A, et al. (2009) Efficacy of bispectral index monitoring as an adjunct to propofol deep sedation for ERCP: a randomized controlled trial. Endoscopy 41: 1046–1051. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
