

Women's higher health risks in the obesogenic environment: a gender nutrition approach to metabolic dimorphism with predictive, preventive, and personalised medicine
- PMID: 23311512
- PMCID: PMC3560240
- DOI: 10.1186/1878-5085-4-1
Women's higher health risks in the obesogenic environment: a gender nutrition approach to metabolic dimorphism with predictive, preventive, and personalised medicine
Abstract
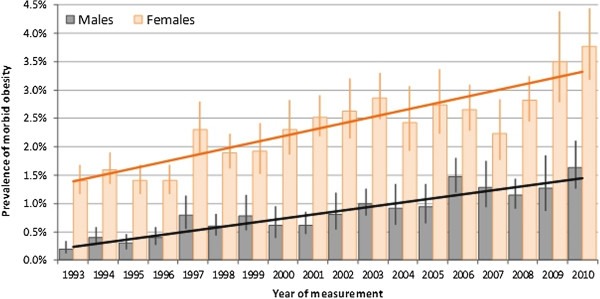
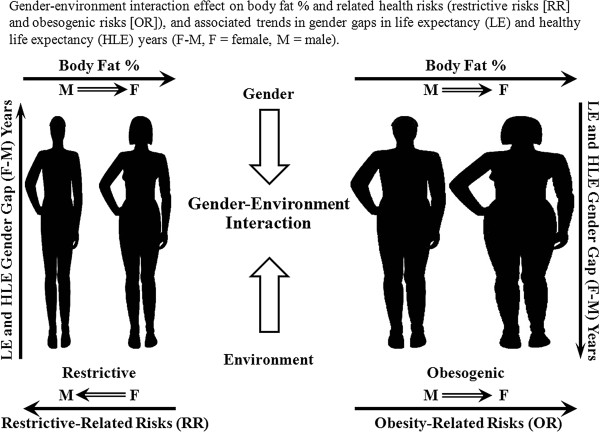
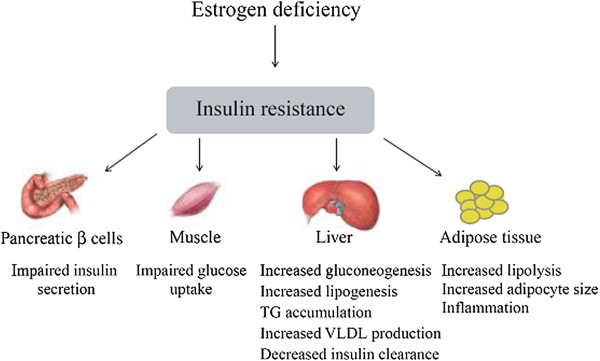
Women's evolution for nurturing and fat accumulation, which historically yielded health and longevity advantages against scarcity, may now be counteracted by increasing risks in the obesogenic environment, recently shown by narrowing gender health gap. Women's differential metabolism/disease risks, i.e. in fat accumulation/distribution, exemplified during puberty/adolescence, suggest gender dimorphism with obesity outcomes. Women's higher body fat percentage than men, even with equal body mass index, may be a better risk predictor. Differential metabolic responses to weight-reduction diets, with women's lower abdominal fat loss, better response to high-protein vs. high-carbohydrate diets, higher risks with sedentariness vs. exercise benefits, and tendency toward delayed manifestation of central obesity, metabolic syndrome, diabetes, cardiovascular disease, and certain cancers until menopause-but accelerated thereafter-suggest a need for differing metabolic and chronological perspectives for prevention/intervention. These perspectives, including women's differential responses to lifestyle changes, strongly support further research with a gender nutrition emphasis within predictive, preventive, and personalized medicine.
Figures

Similar articles
-
Gender-planned health services.Ann Trop Med Parasitol. 1992 Aug;86 Suppl 1:19-23. doi: 10.1080/00034983.1992.11812731. Ann Trop Med Parasitol. 1992. PMID: 1489242
-
Offspring body size and metabolic profile - effects of lifestyle intervention in obese pregnant women.Dan Med J. 2014 Jul;61(7):B4893. Dan Med J. 2014. PMID: 25123127 Review.
-
Women's higher risk with N-6 PUFA vs. men's relative advantage: an "N-6 gender nutrition paradox" hypothesis.Isr Med Assoc J. 2012 Jul;14(7):435-41. Isr Med Assoc J. 2012. PMID: 22953621
-
The influence of sex hormones on obesity across the female life span.J Womens Health. 1998 Dec;7(10):1247-56. doi: 10.1089/jwh.1998.7.1247. J Womens Health. 1998. PMID: 9929857 Review.
-
Traversing the menopause: changes in energy expenditure and body composition.Coron Artery Dis. 1998;9(12):799-803. Coron Artery Dis. 1998. PMID: 9894924 Review.
Cited by
-
Cellphone-based devices for bioanalytical sciences.Anal Bioanal Chem. 2014 May;406(14):3263-77. doi: 10.1007/s00216-013-7473-1. Epub 2013 Nov 28. Anal Bioanal Chem. 2014. PMID: 24287630 Free PMC article. Review.
-
Development of biomarker panel to predict, prevent and create treatments tailored to the persons with human papillomavirus-induced cervical precancerous lesions.EPMA J. 2014 Jan 6;5(1):1. doi: 10.1186/1878-5085-5-1. EPMA J. 2014. PMID: 24386936 Free PMC article.
-
Burden of obesity in the Eastern Mediterranean Region: findings from the Global Burden of Disease 2015 study.Int J Public Health. 2018 May;63(Suppl 1):165-176. doi: 10.1007/s00038-017-1002-5. Epub 2017 Aug 3. Int J Public Health. 2018. PMID: 28776243 Free PMC article.
-
The potential contribution of dietary factors to breast cancer prevention.Eur J Cancer Prev. 2017 Sep;26(5):385-395. doi: 10.1097/CEJ.0000000000000406. Eur J Cancer Prev. 2017. PMID: 28746163 Free PMC article. Review.
-
Global trends in ischemic stroke burden attributable to high BMI.Medicine (Baltimore). 2024 Nov 8;103(45):e40196. doi: 10.1097/MD.0000000000040196. Medicine (Baltimore). 2024. PMID: 39533588 Free PMC article.
References
-
- Laraia BA, Bodnar LM, Siega-Riz AM. Pregravid body mass index is negatively associated with diet quality during pregnancy. Public Health Nutr. 2007;10:920–926. - PubMed
-
- Makrides M, Gibson RA. Long-chain polyunsaturated fatty acid requirements during pregnancy and lactation. Am J Clin Nutr. 2000;71:307S–311S. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
