

Interdisciplinary Comprehensive Arm Rehabilitation Evaluation (ICARE): a randomized controlled trial protocol
- PMID: 23311856
- PMCID: PMC3547701
- DOI: 10.1186/1471-2377-13-5
Interdisciplinary Comprehensive Arm Rehabilitation Evaluation (ICARE): a randomized controlled trial protocol
Abstract
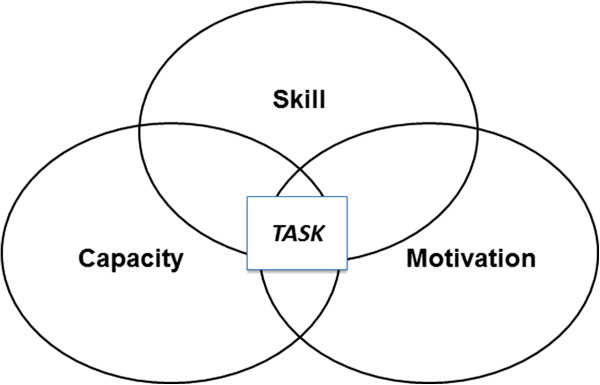
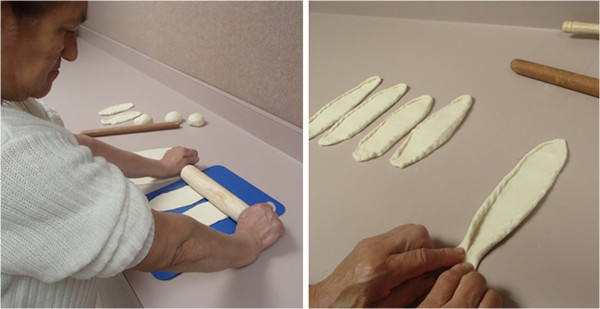
Background: Residual disability after stroke is substantial; 65% of patients at 6 months are unable to incorporate the impaired upper extremity into daily activities. Task-oriented training programs are rapidly being adopted into clinical practice. In the absence of any consensus on the essential elements or dose of task-specific training, an urgent need exists for a well-designed trial to determine the effectiveness of a specific multidimensional task-based program governed by a comprehensive set of evidence-based principles. The Interdisciplinary Comprehensive Arm Rehabilitation Evaluation (ICARE) Stroke Initiative is a parallel group, three-arm, single blind, superiority randomized controlled trial of a theoretically-defensible, upper extremity rehabilitation program provided in the outpatient setting.The primary objective of ICARE is to determine if there is a greater improvement in arm and hand recovery one year after randomization in participants receiving a structured training program termed Accelerated Skill Acquisition Program (ASAP), compared to participants receiving usual and customary therapy of an equivalent dose (DEUCC). Two secondary objectives are to compare ASAP to a true (active monitoring only) usual and customary (UCC) therapy group and to compare DEUCC and UCC.
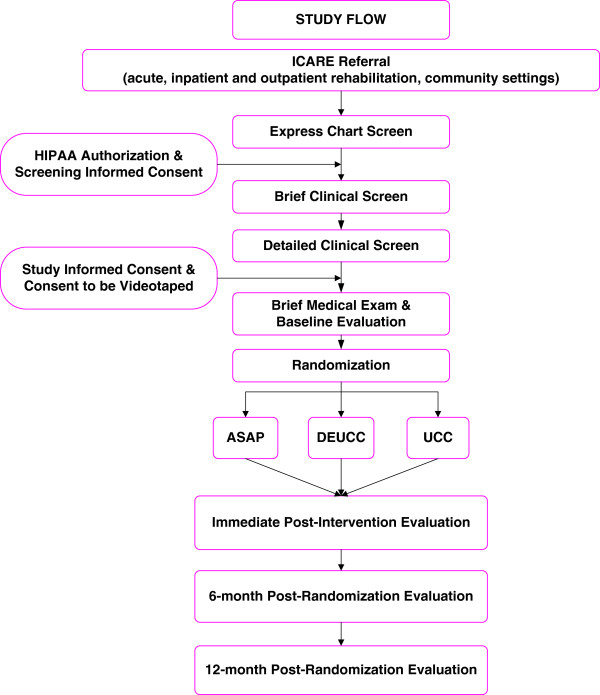
Methods/design: Following baseline assessment, participants are randomized by site, stratified for stroke duration and motor severity. 360 adults will be randomized, 14 to 106 days following ischemic or hemorrhagic stroke onset, with mild to moderate upper extremity impairment, recruited at sites in Atlanta, Los Angeles and Washington, D.C. The Wolf Motor Function Test (WMFT) time score is the primary outcome at 1 year post-randomization. The Stroke Impact Scale (SIS) hand domain is a secondary outcome measure.The design includes concealed allocation during recruitment, screening and baseline, blinded outcome assessment and intention to treat analyses. Our primary hypothesis is that the improvement in log-transformed WMFT time will be greater for the ASAP than the DEUCC group. This pre-planned hypothesis will be tested at a significance level of 0.05.
Discussion: ICARE will test whether ASAP is superior to the same number of hours of usual therapy. Pre-specified secondary analyses will test whether 30 hours of usual therapy is superior to current usual and customary therapy not controlled for dose.
Trial registration: www.ClinicalTrials.gov Identifier: NCT00871715
Figures
References
-
- Gresham GE, Duncan PW, Stason WB, Adams HP, Jr, Adelman AM, Alexander DN, Bishop DS, Diller L, Donaldson NE, Granger CV, Post-Stroke Rehabilitation. Rockville, MD: U.S. Department of Health and Human Services; 1995.
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
