

External validation and comparison with other models of the International Metastatic Renal-Cell Carcinoma Database Consortium prognostic model: a population-based study
- PMID: 23312463
- PMCID: PMC4144042
- DOI: 10.1016/S1470-2045(12)70559-4
External validation and comparison with other models of the International Metastatic Renal-Cell Carcinoma Database Consortium prognostic model: a population-based study
Abstract
Background: The International Metastatic Renal-Cell Carcinoma Database Consortium model offers prognostic information for patients with metastatic renal-cell carcinoma. We tested the accuracy of the model in an external population and compared it with other prognostic models.
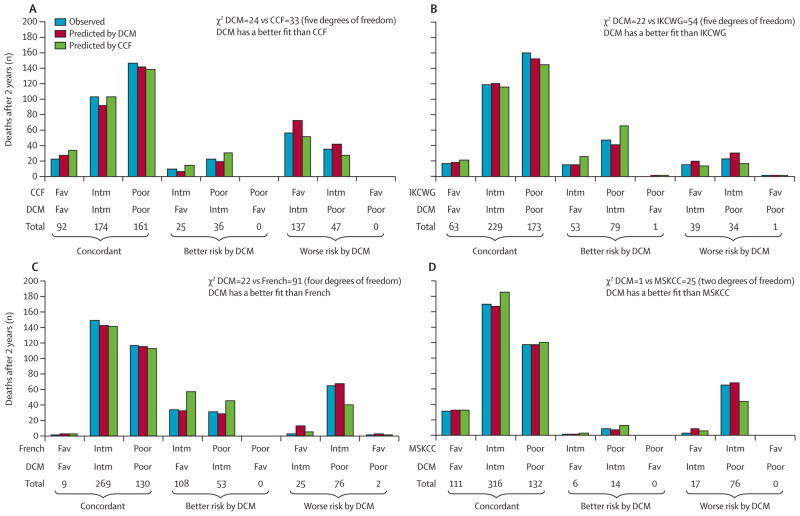
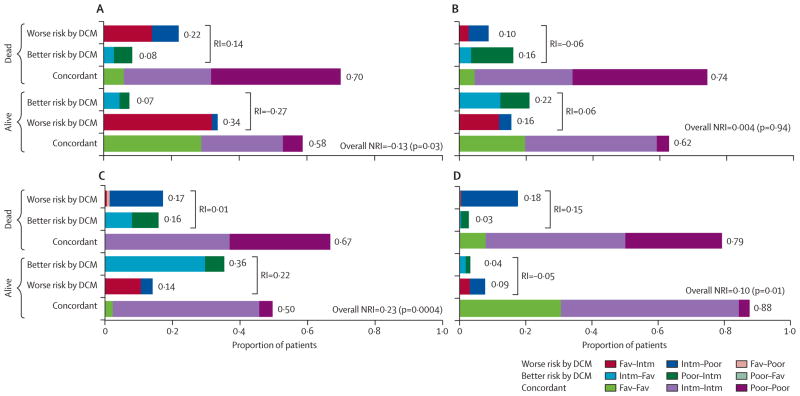
Methods: We included patients with metastatic renal-cell carcinoma who were treated with first-line VEGF-targeted treatment at 13 international cancer centres and who were registered in the Consortium's database but had not contributed to the initial development of the Consortium Database model. The primary endpoint was overall survival. We compared the Database Consortium model with the Cleveland Clinic Foundation (CCF) model, the International Kidney Cancer Working Group (IKCWG) model, the French model, and the Memorial Sloan-Kettering Cancer Center (MSKCC) model by concordance indices and other measures of model fit.
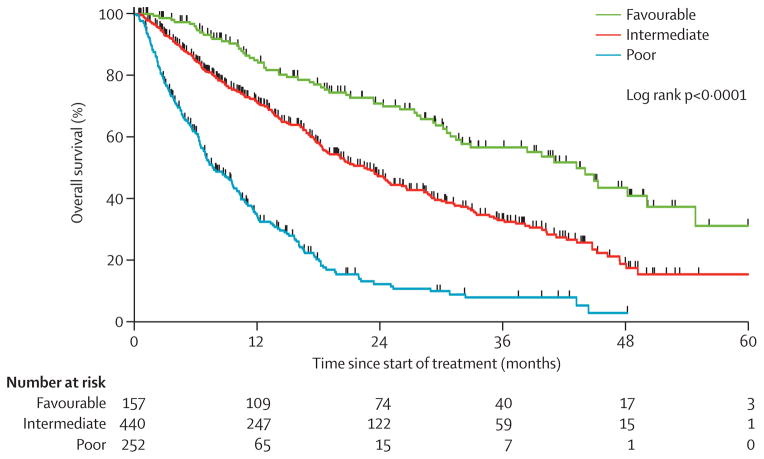
Findings: Overall, 1028 patients were included in this study, of whom 849 had complete data to assess the Database Consortium model. Median overall survival was 18·8 months (95% 17·6-21·4). The predefined Database Consortium risk factors (anaemia, thrombocytosis, neutrophilia, hypercalcaemia, Karnofsky performance status <80%, and <1 year from diagnosis to treatment) were independent predictors of poor overall survival in the external validation set (hazard ratios ranged between 1·27 and 2·08, concordance index 0·71, 95% CI 0·68-0·73). When patients were segregated into three risk categories, median overall survival was 43·2 months (95% CI 31·4-50·1) in the favourable risk group (no risk factors; 157 patients), 22·5 months (18·7-25·1) in the intermediate risk group (one to two risk factors; 440 patients), and 7·8 months (6·5-9·7) in the poor risk group (three or more risk factors; 252 patients; p<0·0001; concordance index 0·664, 95% CI 0·639-0·689). 672 patients had complete data to test all five models. The concordance index of the CCF model was 0·662 (95% CI 0·636-0·687), of the French model 0·640 (0·614-0·665), of the IKCWG model 0·668 (0·645-0·692), and of the MSKCC model 0·657 (0·632-0·682). The reported versus predicted number of deaths at 2 years was most similar in the Database Consortium model compared with the other models.
Interpretation: The Database Consortium model is now externally validated and can be applied to stratify patients by risk in clinical trials and to counsel patients about prognosis.
Funding: None.
Copyright © 2013 Elsevier Ltd. All rights reserved.
Conflict of interest statement
DYCH has an advisory role at Aveo, Pfizer, Novartis, and Bayer. LCH has an advisory role at Novartis and Pfizer and has received research funding from Bristol-Myers Squibb, Novartis, and Genentech. GAB has a consultant and advisory role at Pfizer and has received honoraria and research funding from Pfizer. MM has an advisory role at Novartis and Pfizer and has received research funding from both. LW has an advisory role at Pfizer and Novartis and has received research funding from Pfizer, Novartis, and GlaxoSmithKline. UNV has received honoraria and research funding from Pfizer, Novartis, and GlaxoSmithKline. S-YR has an advisory role at Novartis, Pfizer, and GlaxoSmithKline, and has received research funding from Novartis and Bayer Korea. FD has received research funding from Novartis. CK has an advisory role at Pfizer, Novartis, and GlaxoSmithKline and has received honoraria and research funding from Pfizer, Novartis, and GlaxoSmithKline. BIR has an advisory role at Pfizer, GlaxoSmithKline, Aveo, Bayer, Onyx, and has received research funding from GlaxoSmithKline and Pfizer. TKC has received research funding from Pfizer and has an advisory role at Aveo, Pfizer, Novartis, GlaxoSmithKline, Genentech, Bayer, and Onyx. WX, MMR, M-HT, and NA declare that they have no conflicts of interest.
Figures
Comment in
-
A prognostic model for metastatic renal-cell carcinoma.Lancet Oncol. 2013 Feb;14(2):102-3. doi: 10.1016/S1470-2045(12)70581-8. Epub 2013 Jan 9. Lancet Oncol. 2013. PMID: 23312462 No abstract available.
References
-
- Motzer RJ, Hutson TE, Tomczak P, et al. Sunitinib versus interferon alfa in metastatic renal-cell carcinoma. N Engl J Med. 2007;356:115–24. - PubMed
-
- Escudier B, Eisen T, Stadler WM, et al. Sorafenib in advanced clear-cell renal-cell carcinoma. N Engl J Med. 2007;356:125–34. - PubMed
-
- Escudier B, Pluzanska A, Koralewski P, et al. Bevacizumab plus interferon alfa-2a for treatment of metastatic renal cell carcinoma: a randomised, double-blind phase III trial. Lancet. 2007;370:2103–11. - PubMed
-
- Sternberg CN, Szczylik C, Lee E, et al. A randomized, double-blind phase III study of pazopanib in treatment-naive and cytokine-pretreated patients with advanced renal cell carcinoma (RCC) Proc Am Soc Clin Oncol. 2009;27(suppl):abstr 5021.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
