

Prostate cancer risk inflation as a consequence of image-targeted biopsy of the prostate: a computer simulation study
- PMID: 23312572
- PMCID: PMC3925797
- DOI: 10.1016/j.eururo.2012.12.057
Prostate cancer risk inflation as a consequence of image-targeted biopsy of the prostate: a computer simulation study
Abstract
Background: Prostate biopsy parameters are commonly used to attribute cancer risk. A targeted approach to lesions found on imaging may have an impact on the risk attribution given to a man.
Objective: To evaluate whether, based on computer simulation, targeting of lesions during biopsy results in reclassification of cancer risk when compared with transrectal ultrasound (TRUS) guided biopsy.
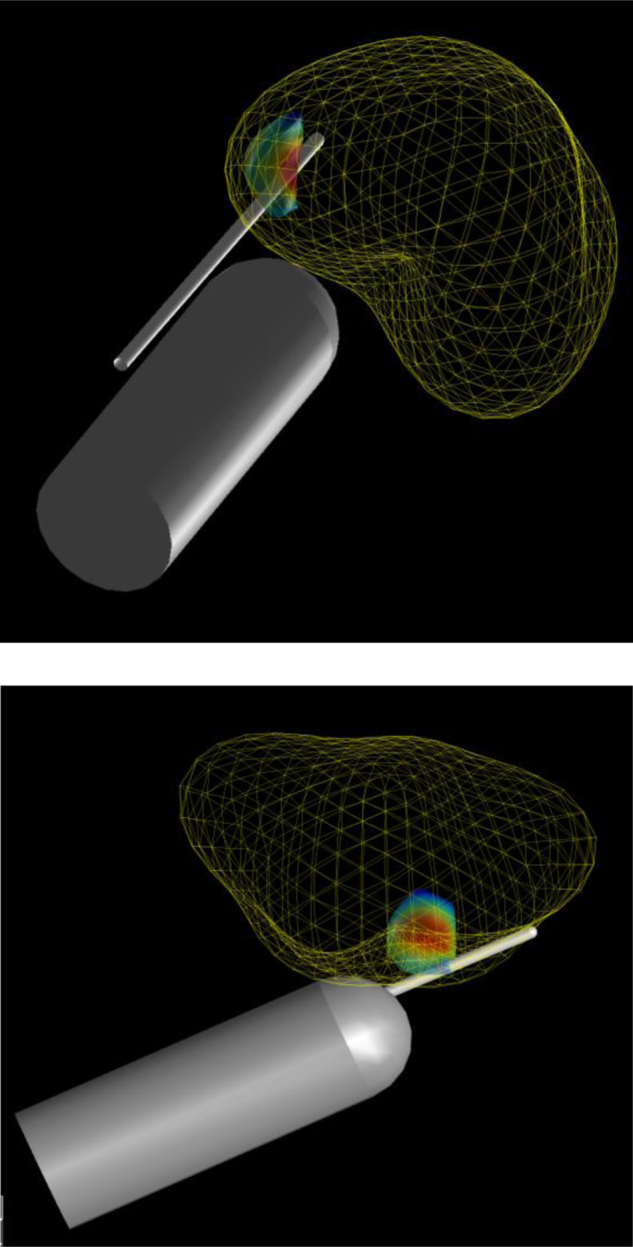
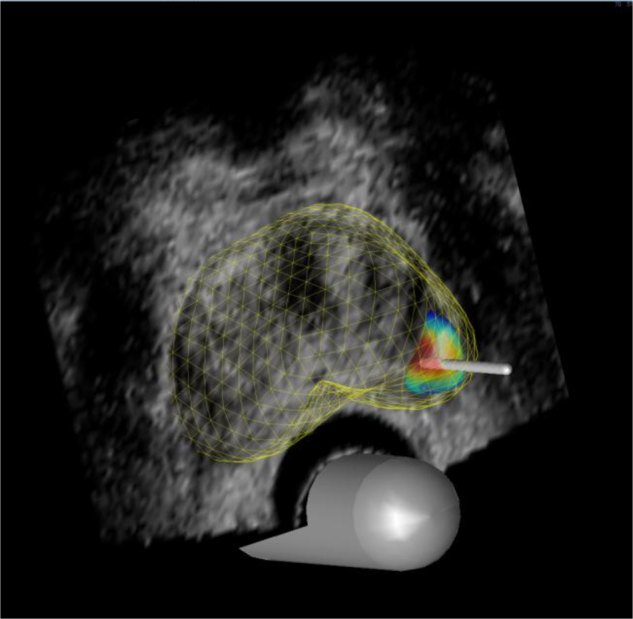
Design, setting, and participants: A total of 107 reconstructed three-dimensional models of whole-mount radical prostatectomy specimens were used for computer simulations. Systematic 12-core TRUS biopsy was compared with transperineal targeted biopsies using between one and five cores. All biopsy strategies incorporated operator and needle deflection error. A target was defined as any lesion ≥ 0.2 ml. A false-positive magnetic resonance imaging identification rate of 34% was applied.
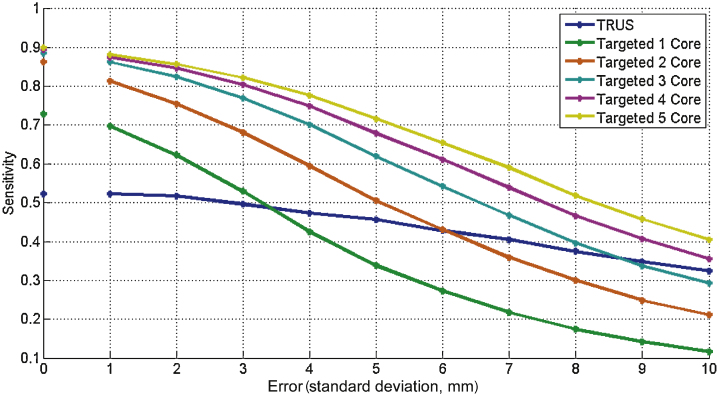
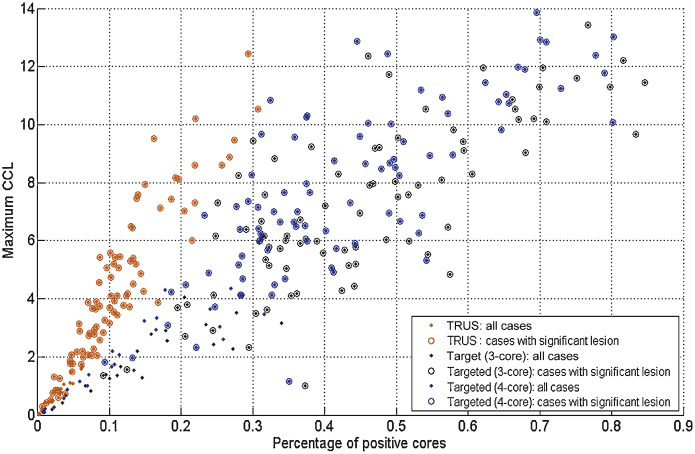
Outcome measurements and statistical analysis: Sensitivity was calculated for the detection of all cancer and clinically significant disease. Cases were designated as high risk based on achieving ≥ 6 mm cancer length and/or ≥ 50% positive cores. Statistical significance (p values) was calculated using both a paired Kolmogorov-Smirnov test and the t test.
Results and limitations: When applying a widely used biopsy criteria to designate risk, 12-core TRUS biopsy classified only 24% (20 of 85) of clinically significant cases as high risk, compared with 74% (63 of 85) of cases using 4 targeted cores. The targeted strategy reported a significantly higher proportion of positive cores (44% vs 11%; p<0.0001) and a significantly greater mean maximum cancer core length (7.8mm vs 4.3mm; p<0.0001) when compared with 12-core TRUS biopsy. Computer simulations may not reflect the sources of errors encountered in clinical practice. To mitigate this we incorporated all known major sources of error to maximise clinical relevance.
Conclusions: Image-targeted biopsy results in an increase in risk attribution if traditional criteria, based on cancer core length and the proportion of positive cores, are applied. Targeted biopsy strategies will require new risk stratification models that account for the increased likelihood of sampling the tumour.
Keywords: Biopsy; Prostate; Risk; Simulation.
Crown Copyright © 2012. Published by Elsevier B.V. All rights reserved.
Figures
References
-
- Ahmed H.U., Emberton M., Kepner G., Kepner J. A biomedical engineering approach to mitigate the errors of prostate biopsy. Nature Rev Urol. 2012;9:227–231. - PubMed
-
- King C.R., McNeal J.E., Gill H. Extended prostate biopsy scheme improves reliability of Gleason grading for radiotherapy patients. Int J Radiat Oncol Biol Phys. 2004;59:386–391. - PubMed
-
- Moore C.M., Robertson N.L., Arsanious N. Image-guided prostate biopsy using magnetic resonance imaging-derived targets: a systematic review. Eur Urol. 2013;63:125–140. - PubMed
-
- Pinto F., Totaro A., Calarco A. Imaging in prostate cancer diagnosis: present role and future perspectives. Urol Int. 2011;86:373–382. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
