

Rehabilitation robotics
- PMID: 23312648
- PMCID: PMC4688009
- DOI: 10.1016/B978-0-444-52901-5.00023-X
Rehabilitation robotics
Abstract
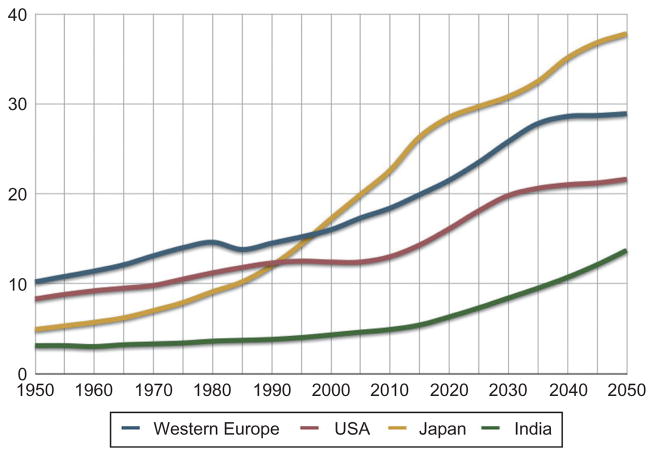
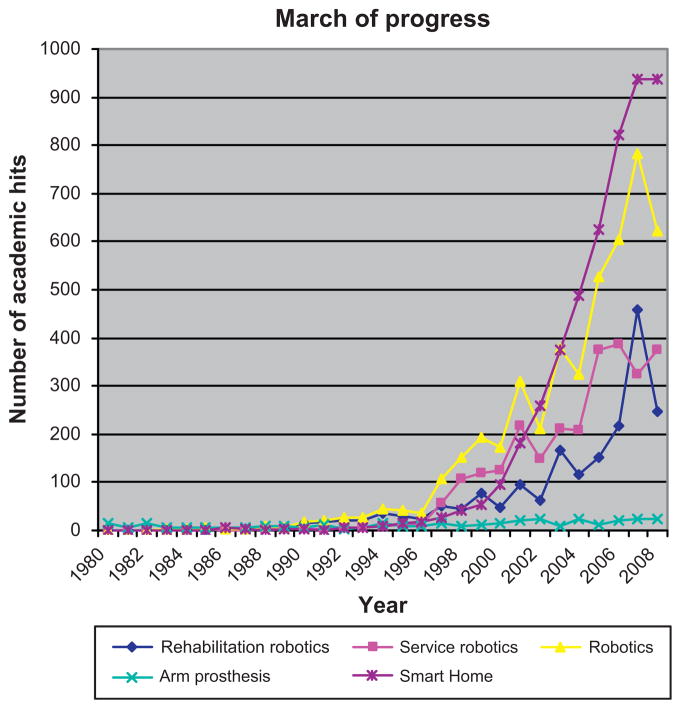
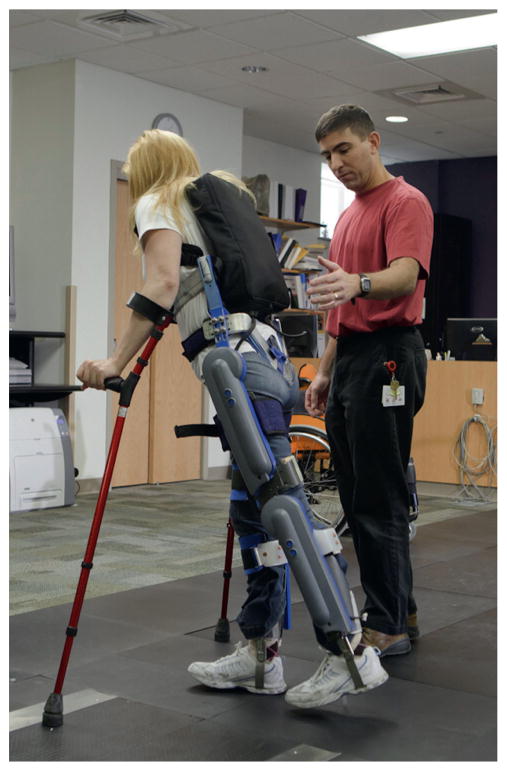
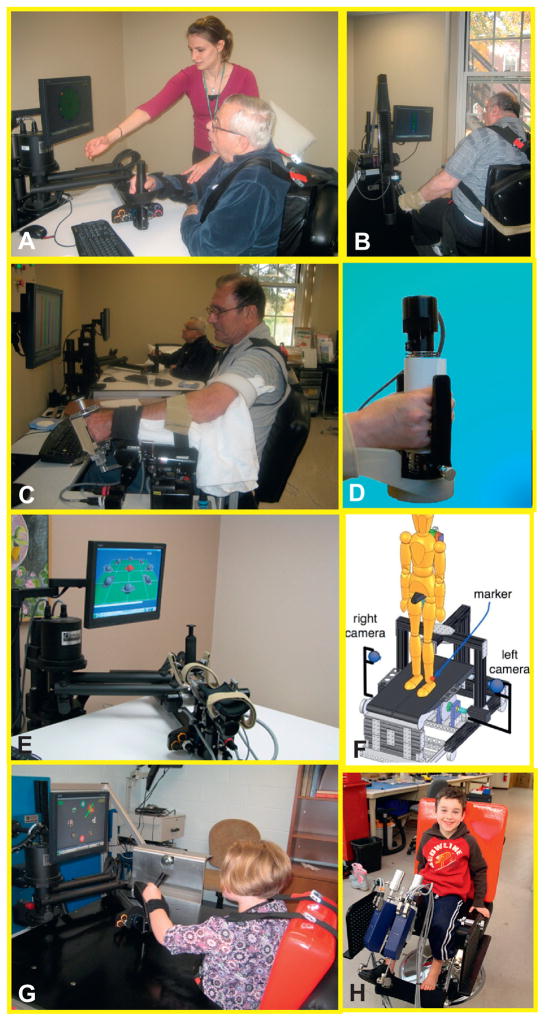
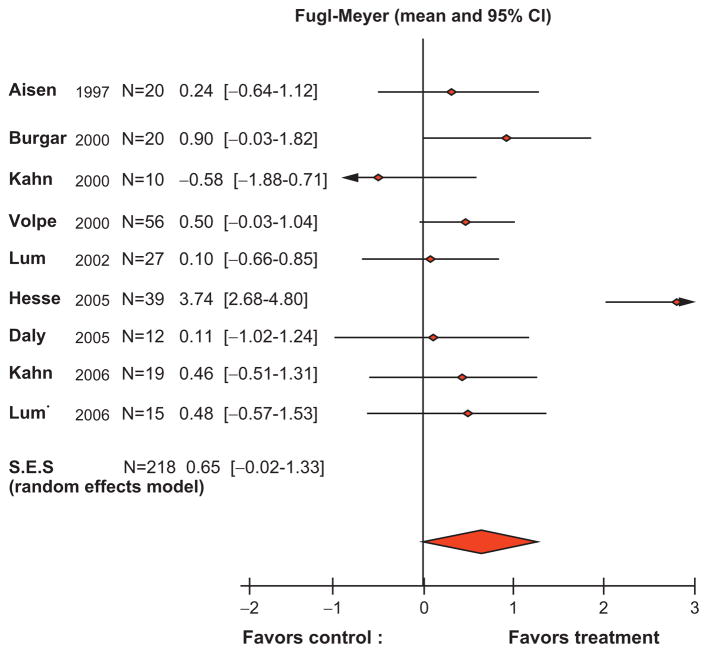
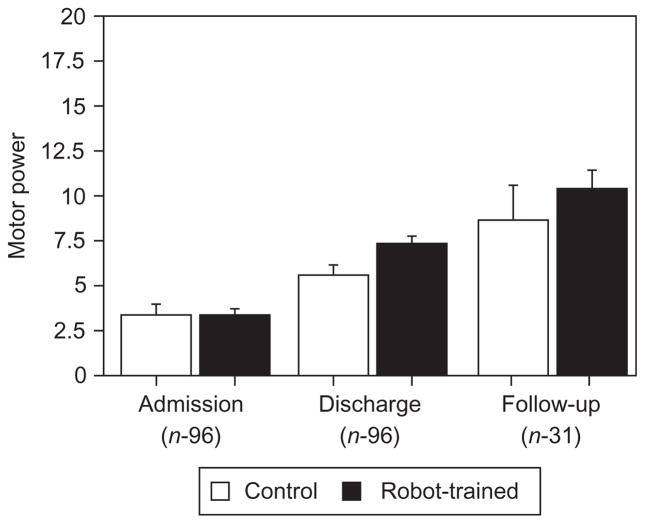
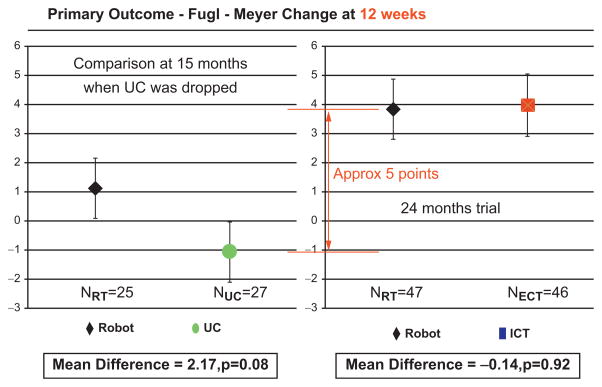
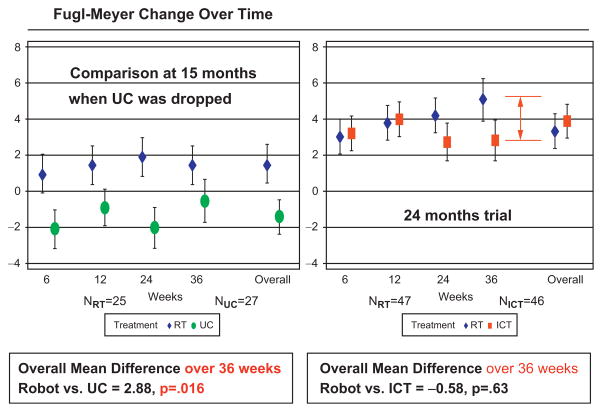
This chapter focuses on rehabilitation robotics which can be used to augment the clinician's toolbox in order to deliver meaningful restorative therapy for an aging population, as well as on advances in orthotics to augment an individual's functional abilities beyond neurorestoration potential. The interest in rehabilitation robotics and orthotics is increasing steadily with marked growth in the last 10 years. This growth is understandable in view of the increased demand for caregivers and rehabilitation services escalating apace with the graying of the population. We provide an overview on improving function in people with a weak limb due to a neurological disorder who cannot properly control it to interact with the environment (orthotics); we then focus on tools to assist the clinician in promoting rehabilitation of an individual so that s/he can interact with the environment unassisted (rehabilitation robotics). We present a few clinical results occurring immediately poststroke as well as during the chronic phase that demonstrate superior gains for the upper extremity when employing rehabilitation robotics instead of usual care. These include the landmark VA-ROBOTICS multisite, randomized clinical study which demonstrates clinical gains for chronic stroke that go beyond usual care at no additional cost.
Copyright © 2013 Elsevier B.V. All rights reserved.
Figures


References
-
- Aisen ML, Krebs HI, Hogan N, et al. The effect of robot-assisted therapy and rehabilitative training on motor recovery following stroke. Arch Neurol. 1997;54:443–446. - PubMed
-
- American Heart Association. Heart Disease and Stroke Statistics – 2010 Update 2010
-
- Brashear A, Gordon MF, Elovi E, et al. Intramuscular injection of botulinun toxin for the treatment of wrist and finger spasticity after a stroke. N Engl J Med. 2002;347:395–400. - PubMed
-
- Butler P, Major R, Patrick J. The technique of reciprocal walking using the hip guidance orthosis (HGO) with crutches. Prosthet Orthot Int. 1984;8:33–38. - PubMed
-
- Duncan PW, Bode RK, Min Lai S. Analysis of a new stroke-specific outcome scale: the Stroke Impact Scale. Arch Phys Med Rehabil. 2003;84:950–963. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
