

Immunosuppression for progressive membranous nephropathy: a UK randomised controlled trial
- PMID: 23312808
- PMCID: PMC3590447
- DOI: 10.1016/S0140-6736(12)61566-9
Immunosuppression for progressive membranous nephropathy: a UK randomised controlled trial
Abstract
Background: Membranous nephropathy leads to end-stage renal disease in more than 20% of patients. Although immunosuppressive therapy benefits some patients, trial evidence for the subset of patients with declining renal function is not available. We aimed to assess whether immunosuppression preserves renal function in patients with idiopathic membranous nephropathy with declining renal function.
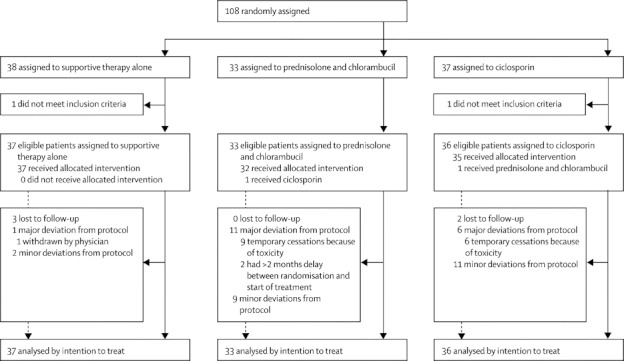
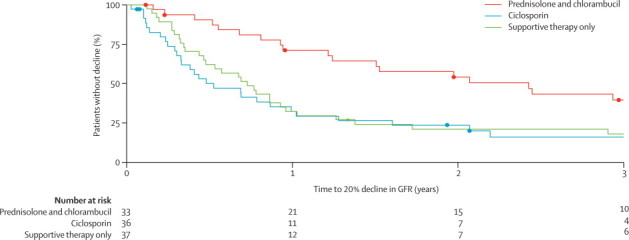
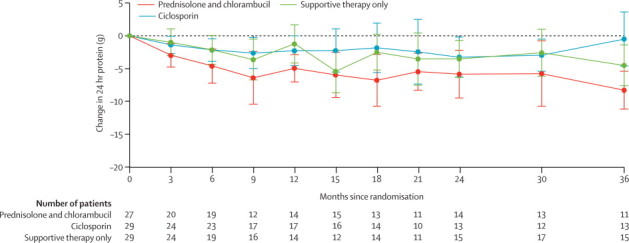
Methods: This randomised controlled trial was undertaken in 37 renal units across the UK. We recruited patients (18-75 years) with biopsy-proven idiopathic membranous nephropathy, a plasma creatinine concentration of less than 300 μmol/L, and at least a 20% decline in excretory renal function measured in the 2 years before study entry, based on at least three measurements over a period of 3 months or longer. Patients were randomly assigned (1:1:1) by a random number table to receive supportive treatment only, supportive treatment plus 6 months of alternating cycles of prednisolone and chlorambucil, or supportive treatment plus 12 months of ciclosporin. The primary outcome was a further 20% decline in renal function from baseline, analysed by intention to treat. The trial is registered as an International Standard Randomised Controlled Trial, number 99959692.
Findings: We randomly assigned 108 patients, 33 of whom received prednisolone and chlorambucil, 37 ciclosporin, and 38 supportive therapy alone. Two patients (one who received ciclosporin and one who received supportive therapy) were ineligible, so were not included in the intention-to-treat analysis, and 45 patients deviated from protocol before study end, mostly as a result of minor dose adjustments. Follow up was until primary endpoint or for minimum of 3 years if primary endpoint was not reached. Risk of further 20% decline in renal function was significantly lower in the prednisolone and chlorambucil group than in the supportive care group (19 [58%] of 33 patients reached endpoint vs 31 [84%] of 37, hazard ratio [HR] 0·44 [95% CI 0·24-0·78]; p=0·0042); risk did not differ between the ciclosporin (29 [81%] of 36) and supportive treatment only groups (HR 1·17 [0·70-1·95]; p=0·54), but did differ significantly across all three groups (p=0·003). Serious adverse events were frequent in all three groups but were higher in the prednisolone and chlorambucil group than in the supportive care only group (56 events vs 24 events; p=0·048).
Interpretation: For the subset of patients with idiopathic membranous nephropathy and deteriorating excretory renal function, 6 months' therapy with prednisolone and chlorambucil is the treatment approach best supported by our evidence. Ciclosporin should be avoided in this subset.
Funding: Medical Research Council, Novartis, Renal Association, Kidney Research UK.
Copyright © 2013 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
Idiopathic membranous nephropathy: back to the future?Lancet. 2013 Mar 2;381(9868):706-8. doi: 10.1016/S0140-6736(12)62033-9. Epub 2013 Jan 9. Lancet. 2013. PMID: 23312809 No abstract available.
-
Glomerular disease: An RCT of treatment for idiopathic membranous nephropathy.Nat Rev Nephrol. 2013 Mar;9(3):126. doi: 10.1038/nrneph.2013.11. Epub 2013 Jan 29. Nat Rev Nephrol. 2013. PMID: 23358422 No abstract available.
-
ACP Journal Club. Prednisolone plus chlorambucil preserved renal function in membranous nephropathy.Ann Intern Med. 2013 May 21;158(10):JC9. doi: 10.7326/0003-4819-158-10-201305210-02009. Ann Intern Med. 2013. PMID: 23689788 No abstract available.
-
Immunosuppression for membranous nephropathy.Lancet. 2013 Jun 22;381(9884):2161. doi: 10.1016/S0140-6736(13)61432-4. Lancet. 2013. PMID: 23791336 No abstract available.
-
Immunosuppression for membranous nephropathy.Lancet. 2013 Jun 22;381(9884):2161. doi: 10.1016/S0140-6736(13)61431-2. Lancet. 2013. PMID: 23791337 No abstract available.
-
Immunosuppression for membranous nephropathy.Lancet. 2013 Jun 22;381(9884):2161-2. doi: 10.1016/S0140-6736(13)61433-6. Lancet. 2013. PMID: 23791338 No abstract available.
-
Immunosuppression for membranous nephropathy.Lancet. 2013 Jun 22;381(9884):2162-3. doi: 10.1016/S0140-6736(13)61435-X. Lancet. 2013. PMID: 23791339 No abstract available.
-
Immunosuppression for membranous nephropathy.Lancet. 2013 Jun 22;381(9884):2162. doi: 10.1016/S0140-6736(13)61434-8. Lancet. 2013. PMID: 23791340 No abstract available.
-
Immunosuppression for membranous nephropathy - Authors' reply.Lancet. 2013 Jun 22;381(9884):2163. doi: 10.1016/S0140-6736(13)61436-1. Lancet. 2013. PMID: 23791342 No abstract available.
References
-
- Hofstra JM, Wetzels JF. Introduction of a cyclophosphamide-based treatment strategy and the risk of ESRD in patients with idiopathic membranous nephropathy: a nationwide survey in the Netherlands. Nephrol Dial Transplant. 2008;23:3534–3538. - PubMed
-
- National Kidney and Urologic Diseases Information Clearinghouse (NKUDIC) Kidney Disease Statistics for the United States. http://kidney.niddk.nih.gov/kudiseases/pubs/kustats/ (accessed Sept 9, 2012).
-
- Donadio JV, Jr, Torres VE, Velosa JA. Idiopathic membranous nephropathy: the natural history of untreated patients. Kidney Int. 1988;33:708–715. - PubMed
-
- Mathieson PW, Rees AJ. A critical review of treatment for membranous nephropathy. Adv Nephrol Necker Hosp. 1991;20:151–174. - PubMed
-
- Davison AM, Cameron JS, Kerr DN, Ogg CS, Wilkinson RW. The natural history of renal function in untreated idiopathic membranous glomerulonephritis in adults. Clin Nephrol. 1984;22:61–67. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
