

Prosthetic graft infections involving the femoral artery
- PMID: 23312940
- PMCID: PMC3587316
- DOI: 10.1016/j.jvs.2012.09.049
Prosthetic graft infections involving the femoral artery
Abstract
Background: Prosthetic graft infection is a major complication of peripheral vascular surgery. We investigated the experience of a single institution over 10 years with bypass grafts involving the femoral artery to determine the incidence and risk factors for prosthetic graft infection.
Methods: A retrospective cohort single-institution review of prosthetic bypass grafts involving the femoral artery from 2001 to 2010 evaluated patient demographics, body mass index, comorbidities, indications, location of bypass, type of prosthetic material, case urgency, and previous ipsilateral bypass or percutaneous interventions and evaluated the incidence of graft infections, amputations, and mortality.
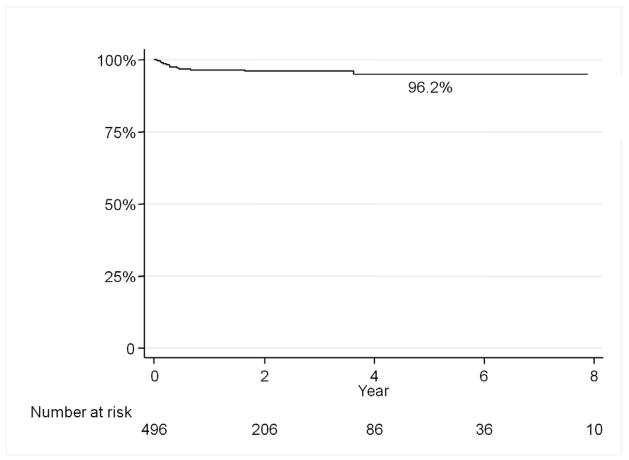
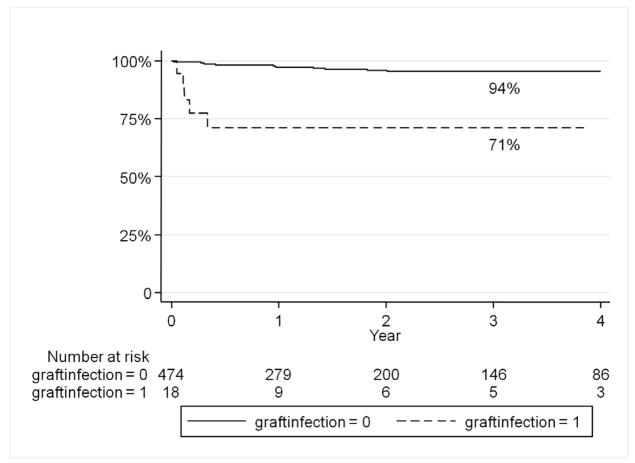
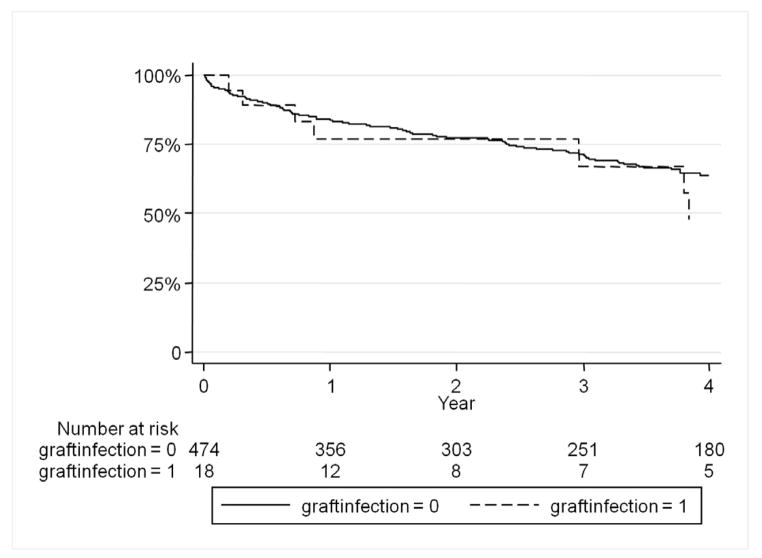
Results: There were 496 prosthetic grafts identified with a graft infection rate of 3.8% (n = 19) at a mean follow-up of 27 months. Multivariable analysis showed that redo bypass (hazard ratio [HR], 5.8; 95% confidence interval [CI], 2.2-15.0), active infection at the time of bypass (HR, 5.2; 95% CI, 1.9-14.2), female gender (HR, 4.5; 95% CI, 1.6-12.7), and diabetes mellitus (HR, 4.6; 95% CI, 1.5-14.3) were significant predictors of graft infection. Graft infection was predictive of major lower extremity amputation (HR, 9.8; 95% CI, 3.5-27.1), as was preoperative tissue loss (HR, 4.7; 95% CI, 1.8-11.9). Graft infection did not predict long-term mortality; however, chronic renal insufficiency (HR, 2.3; 95% CI, 1.6-3.4), tissue loss (HR, 1.4; 95% CI, 1.0-1.9), and active infection (HR, 2.3; 95% CI, 1.6-3.4) did. Infected grafts were removed 79% of the time. Staphylococcus epidermidis (37%) and methicillin-sensitive Staphylococcus aureus (26%) were the most common pathogens isolated.
Conclusions: Redo bypass, female gender, diabetes, and active infection at the time of bypass are associated with a higher risk for prosthetic graft infection and major extremity amputation but do not confer an increased risk of mortality. Autologous vein for lower extremity bypass and endovascular interventions should be considered when feasible in high-risk patients.
Copyright © 2013 Society for Vascular Surgery. Published by Mosby, Inc. All rights reserved.
Figures
References
-
- Siracuse JJ, Giles KA, Pomposelli FB, Hamdan AD, Wyers MC, Chaikof EL, Nedeau AE, Schermerhorn ML. Long-term results for primary bypass versus primary angioplasty/stent for intermittent claudication due to superficial femoral artery occlusive disease. J Vasc Surg. 2012 Apr;55(4):1001–7. Epub 2012 Feb 1. - PMC - PubMed
-
- Greenblatt DY, Rajamanickam V, Mell MW. Predictors of surgical site infection after open lower extremity revascularization. J Vasc Surg. 2011 Aug;54(2):433–9. Epub 2011 Mar 31. - PubMed
-
- Edwards WH, Jr, Martin RS, 3rd, Jenkins JM, Edwards WH, Sr, Mulherin JL., Jr Primary graft infections. J Vasc Surg. 1987 Sep;6(3):235–9. - PubMed
-
- Chang JK, Calligaro KD, Ryan S, Runyan D, Dougherty MJ, Stern JJ. Risk factors associated with infection of lower extremity revascularization: analysis of 365 procedures performed at a teaching hospital. Ann Vasc Surg. 2003 Jan;17(1):91–6. Epub 2003 Jan 15. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
