

Coronary autoregulation is abnormal in syndrome X: insights using myocardial contrast echocardiography
- PMID: 23313388
- PMCID: PMC3582827
- DOI: 10.1016/j.echo.2012.12.008
Coronary autoregulation is abnormal in syndrome X: insights using myocardial contrast echocardiography
Abstract
Background: Syndrome X in women is thought to be caused by coronary microvascular dysfunction, the exact site of which is unknown. The aim of this study was to characterize the microvascular site of dysfunction in these patients using myocardial contrast echocardiography.
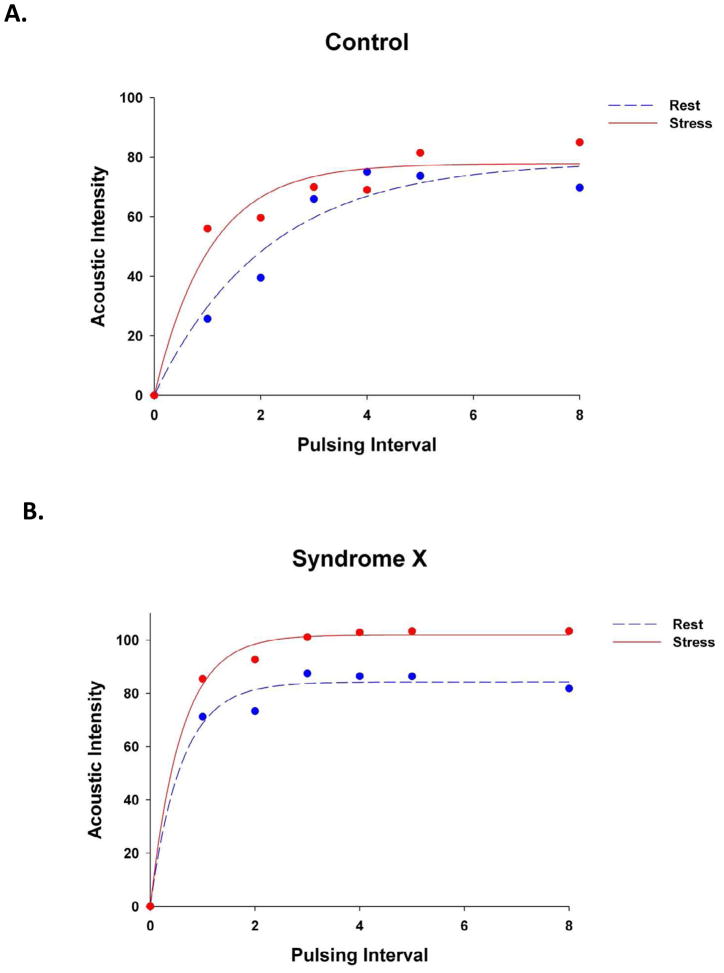
Methods: Women with exertional angina, positive test results on stress imaging, but no coronary artery disease (the study group, n = 18) and age-matched control women also with no coronary artery disease (n = 17) were enrolled. Myocardial contrast echocardiography was performed at rest and during dipyridamole-induced hyperemia. Mean microbubble velocity (β) and myocardial blood volume (A) were measured, and myocardial blood flow (A · β) was computed. In addition, plasma concentrations of eicosanoids, female sex hormones, and C-reactive protein were measured.
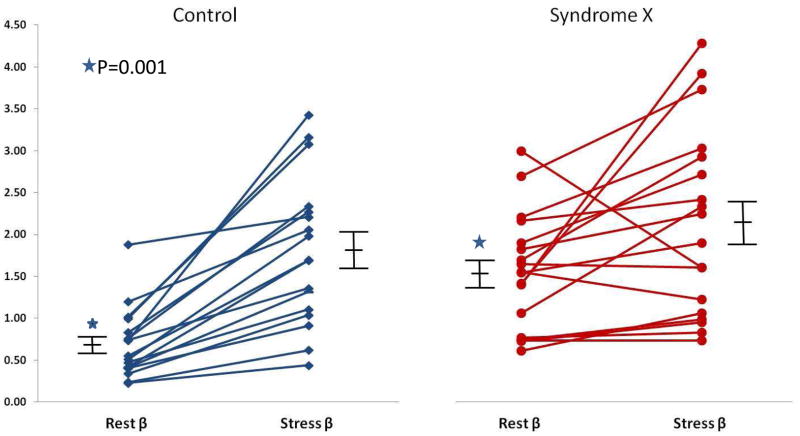
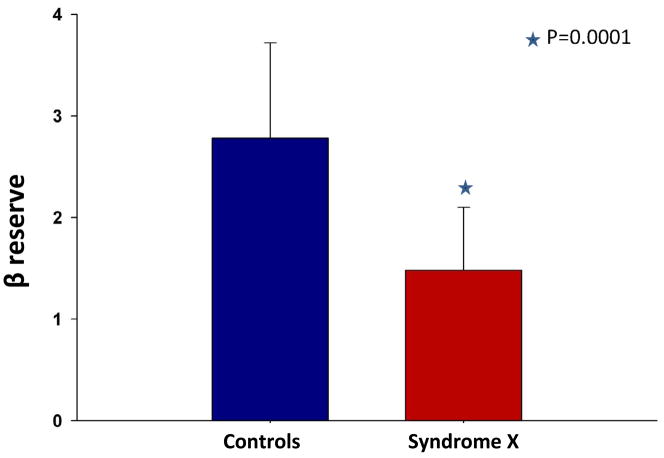
Results: Rest β and myocardial blood flow (A · β) were higher in the study compared with the control women (1.61 ± 0.68 vs. 0.74 ± 0.44, P = .0001, and 157 ± 121 vs. 54 ± 54, P = 0.0001, respectively) despite similar heart rates and systolic blood pressures. After the administration of dipyridamole, whereas the changes in A and A · β were not significantly different between the two groups, β reserve (the ratio of stress β to rest β) was markedly lower in the study group (1.48 ± 0.62 vs. 2.78 ± 0.94, P = .0001). Blood hematocrit, eicosanoids, female sex hormones, glucose, and C-reactive protein were not different between the two groups.
Conclusions: Coronary autoregulation is abnormal in patients with syndrome X (higher resting β and myocardial blood flow and lower β reserve), which suggests that the coronary resistance vessels are the site of microvascular abnormality.
Copyright © 2013 American Society of Echocardiography. Published by Mosby, Inc. All rights reserved.
Figures
References
-
- Kemp HG, Elliott WC, Gorlin R. The angina syndrome with normal coronary arteriography. Trans Assoc Am Physicians. 1967;80:59–70. - PubMed
-
- von Mering GO, Arant CB, Wessel TR, McGorray SP, Bairey Merz CN, et al. Abnormal coronary vasomotion as a prognostic indicator of cardiovascular events in women: results from the National Heart, Lung, and Blood Institute-Sponsored Women's Ischemia Syndrome Evaluation (WISE) Circulation. 2004;109:722–725. - PubMed
-
- Bugiardini R, Manfrini O, Pizzi C, Fontana F, Morgagni G. Endothelial function predicts future development of coronary artery disease: a study of women with chest pain and normal coronary angiograms. Circulation. 2004;109:2518–2523. - PubMed
-
- Cannon RO, 3rd, Epstein SE. “icrovascular angina” as a cause of chest pain with angiographically normal coronary arteries. Am J Cardiol. 1988;61:1338–1343. - PubMed
-
- Cannon RO, 3rd, Watson RM, Rosing DR, Epstein SE. Angina caused by reduced vasodilator reserve of the small coronary arteries. J Am Coll Cardiol. 1983;1:1359–1373. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
