

A comparison of etanercept vs. infliximab for the treatment of post-arrest myocardial dysfunction in a swine model of ventricular fibrillation
- PMID: 23313857
- PMCID: PMC3679243
- DOI: 10.1016/j.resuscitation.2012.12.028
A comparison of etanercept vs. infliximab for the treatment of post-arrest myocardial dysfunction in a swine model of ventricular fibrillation
Abstract
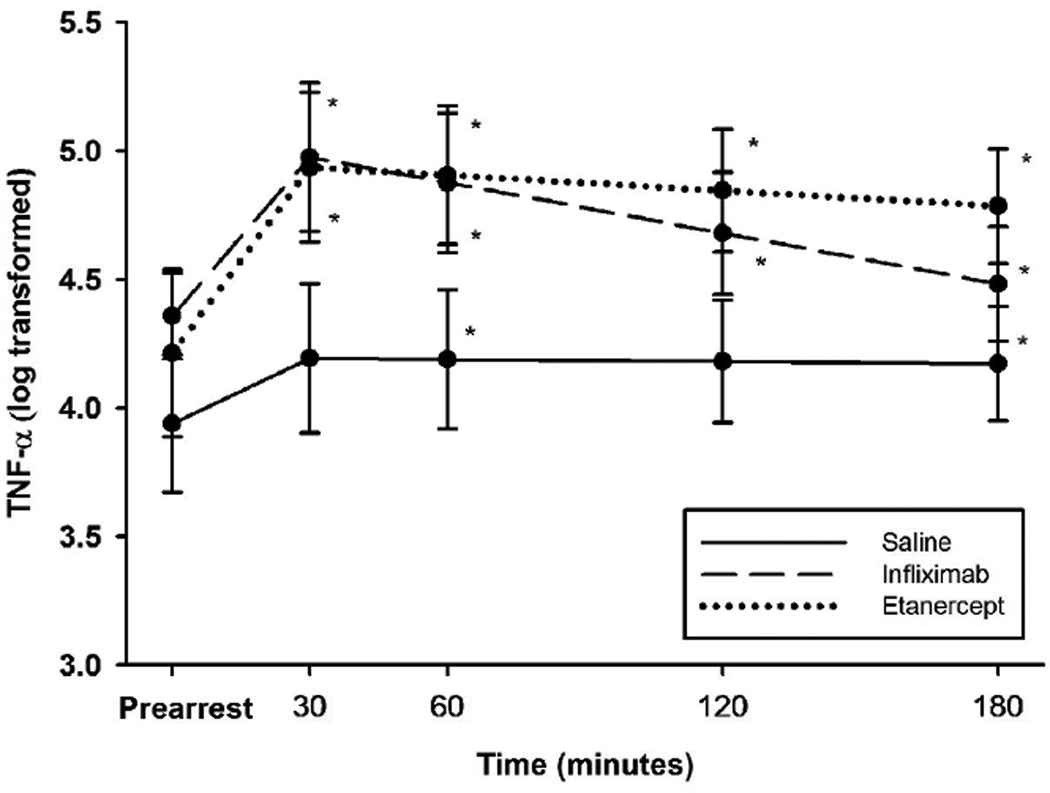
Aims: To compare the effects of two TNF-α antagonists, etanercept and infliximab, on post-cardiac arrest hemodynamics and global left ventricular function (LV) in a swine model following ventricular fibrillation (VF).
Methods: Domestic swine (n=30) were placed under general anesthesia and instrumented before VF was induced electrically. After 7 min of VF, standard ACLS resuscitation was performed. Animals achieving return of spontaneous circulation (ROSC) were randomized to immediately receive infliximab (5 mg/kg, n=10) or etanercept (0.3 mg/kg [4 mg/m(2)], n=10) or vehicle (250 mL normal saline [NS], n=10) and LV function and hemodynamics were monitored for 3 h.
Results: Following ROSC, mean arterial pressure (MAP), stroke work (SW), and LV dP/dt fell from pre-arrest values in all groups. However, at the 30 min nadir, infliximab-treated animals had higher MAP than either the NS group (difference 14.4 mm Hg, 95% confidence interval [CI] 4.2-24.7) or the etanercept group (19.2 mm Hg, 95% CI 9.0-29.5), higher SW than the NS group (10.3 gm-m, 95% CI 5.1-15.5) or the etanercept group (8.9 gm-m, 95% CI 4.0-14.4) and greater LV dP/dt than the NS group (282.9 mm Hg/s, 95% CI 169.6-386.1 higher with infliximab) or the etanercep group (228.9 mm Hg/s, 95% CI 115.6-342.2 higher with infliximab).
Conclusions: Only infliximab demonstrated a beneficial effect on post cardiac arrest hemodynamics and LV function in this swine model. Etanercept was no better in this regard than saline.
Copyright © 2013 Elsevier Ireland Ltd. All rights reserved.
Conflict of interest statement
Conflict of interest statement
The authors report no conflicts of interest.
Figures



Similar articles
-
TNF-α blockade improves early post-resuscitation survival and hemodynamics in a swine model of ischemic ventricular fibrillation.Resuscitation. 2013 Jan;84(1):103-7. doi: 10.1016/j.resuscitation.2012.05.021. Epub 2012 Jun 7. Resuscitation. 2013. PMID: 22683946 Free PMC article.
-
Administration of amiodarone during resuscitation is associated with higher tumor necrosis factor-α levels in the early postarrest period in the swine model of ischemic ventricular fibrillation.J Interferon Cytokine Res. 2013 Jun;33(6):292-6. doi: 10.1089/jir.2012.0123. Epub 2013 May 9. J Interferon Cytokine Res. 2013. PMID: 23659671 Free PMC article.
-
Infliximab attenuates early myocardial dysfunction after resuscitation in a swine cardiac arrest model.Crit Care Med. 2010 Apr;38(4):1162-7. doi: 10.1097/CCM.0b013e3181d44324. Crit Care Med. 2010. PMID: 20154606 Free PMC article.
-
Cardiac function and the proinflammatory cytokine response after recovery from cardiac arrest in swine.J Interferon Cytokine Res. 2009 Nov;29(11):749-58. doi: 10.1089/jir.2009.0035. J Interferon Cytokine Res. 2009. PMID: 19642909 Free PMC article.
-
Fungal infections complicating tumor necrosis factor alpha blockade therapy.Mayo Clin Proc. 2008 Feb;83(2):181-94. Mayo Clin Proc. 2008. PMID: 18241628 Review.
Cited by
-
The relationship between low survival and acute increase of tumor necrosis factor α expression in the lung in a rat model of asphyxial cardiac arrest.Anat Cell Biol. 2018 Jun;51(2):128-135. doi: 10.5115/acb.2018.51.2.128. Epub 2018 Jun 27. Anat Cell Biol. 2018. PMID: 29984058 Free PMC article.
-
Changes in histopathology and tumor necrosis factor-α levels in the hearts of rats following asphyxial cardiac arrest.Clin Exp Emerg Med. 2017 Sep 30;4(3):160-167. doi: 10.15441/ceem.17.220. eCollection 2017 Sep. Clin Exp Emerg Med. 2017. PMID: 29026890 Free PMC article.
-
Neuronal injury and tumor necrosis factor-alpha immunoreactivity in the rat hippocampus in the early period of asphyxia-induced cardiac arrest under normothermia.Neural Regen Res. 2017 Dec;12(12):2007-2013. doi: 10.4103/1673-5374.221157. Neural Regen Res. 2017. PMID: 29323039 Free PMC article.
-
Myocardial Dysfunction and Shock after Cardiac Arrest.Biomed Res Int. 2015;2015:314796. doi: 10.1155/2015/314796. Epub 2015 Sep 2. Biomed Res Int. 2015. PMID: 26421284 Free PMC article. Review.
-
Right ventricular dysfunction after resuscitation predicts poor outcomes in cardiac arrest patients independent of left ventricular function.Resuscitation. 2015 Nov;96:186-91. doi: 10.1016/j.resuscitation.2015.08.008. Epub 2015 Aug 28. Resuscitation. 2015. PMID: 26318576 Free PMC article.
References
-
- Neumar R, Nolan J, Adrie C, et al. Post-cardiac arrest syndrome: epidemiology, pathophysiology, treatment, and prognostication. A consensus statement from the International Liaison Committee on Resuscitation (American Heart Association, Australian and New Zealand Council on Resuscitation, European Resuscitation Council, Heart and Stroke Foundation of Canada, InterAmerican Heart Foundation, Resuscitation Council of Asia, and the Resuscitation Council of Southern Africa); the American Heart Association Emergency Cardiovascular Care Committee; the Council on Cardiovascular Surgery and Anesthesia; the Council on Cardiopulmonary, Perioperative, and Critical Care; the Council on Clinical Cardiology; the Stroke Council. Circulation. 2008;118:2452–2535. - PubMed
-
- Nadkarni VM, Larkin GL, Peberdy MA, et al. First Documented Rhythm and Clinical Outcome From In-Hospital Cardiac Arrest Among Children and Adults. JAMA. 2006;295:50–57. - PubMed
-
- Nolan JP, Laver SR, Welch CA, Harrison DA, Gupta V, Rowan K. Outcome following admission to UK intensive care units after cardiac arrest: a secondary analysis of the ICNARC Case Mix Programme Database*. Anaesthesia. 2007;62:1207–1216. - PubMed
-
- Adrie C. Successful Cardiopulmonary Resuscitation After Cardiac Arrest as a "Sepsis-Like" Syndrome. Circulation. 2002;106:562–568. - PubMed
-
- Ito T, Saitoh D, Fukuzuka K, et al. Significance of elevated serum interleukin-8 in patients resuscitated after cardiopulmonary arrest. Resuscitation. 2001;51:47–100. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
