

A blueprint for the prevention of preterm birth: vaginal progesterone in women with a short cervix
- PMID: 23314512
- PMCID: PMC4151573
- DOI: 10.1515/jpm-2012-0272
A blueprint for the prevention of preterm birth: vaginal progesterone in women with a short cervix
Abstract
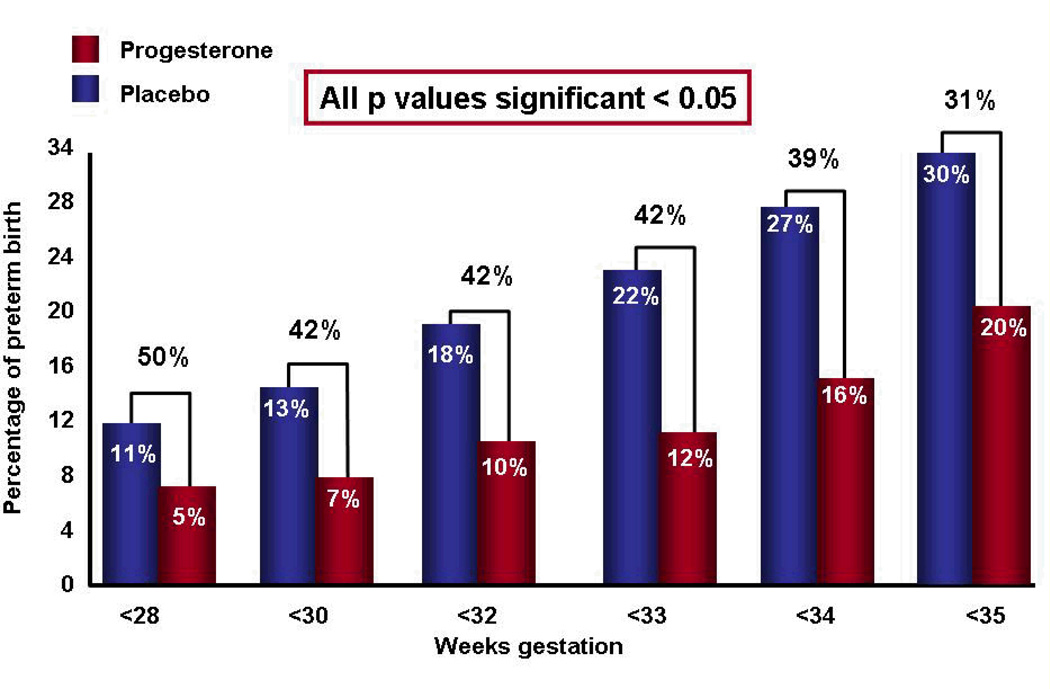
Preterm birth is the leading cause of perinatal morbidity and mortality worldwide, and is the most important challenge to modern obstetrics. A major obstacle has been that preterm birth is treated (implicitly or explicitly) as a single condition. Two thirds of preterm births occur after the spontaneous onset of labor, and the remaining one third after "indicated" preterm birth; however, the causes of spontaneous preterm labor and "indicated" preterm birth are different. Spontaneous preterm birth is a syndrome caused by multiple etiologies, one of which is a decline in progesterone action, which induces cervical ripening. A sonographic short cervix (identified in the midtrimester) is a powerful predictor of spontaneous preterm delivery. Randomized clinical trials and individual patient meta-analyses have shown that vaginal progesterone reduces the rate of preterm delivery at <33 weeks of gestation by 44%, along with the rate of admission to the neonatal intensive care unit, respiratory distress syndrome, requirement for mechanical ventilation, and composite neonatal morbidity/mortality score. There is no evidence that 17-α-hydroxyprogesterone caproate can reduce the rate of preterm delivery in women with a short cervix, and therefore, the compound of choice is natural progesterone (not the synthetic progestin). Routine assessment of the risk of preterm birth with cervical ultrasound coupled with vaginal progesterone for women with a short cervix is cost-effective, and the implementation of such a policy is urgently needed. Vaginal progesterone is as effective as cervical cerclage in reducing the rate of preterm delivery in women with a singleton gestation, history of preterm birth, and a short cervix (<25 mm).
Figures











Similar articles
-
Progesterone to prevent spontaneous preterm birth.Semin Fetal Neonatal Med. 2014 Feb;19(1):15-26. doi: 10.1016/j.siny.2013.10.004. Epub 2013 Dec 5. Semin Fetal Neonatal Med. 2014. PMID: 24315687 Free PMC article. Review.
-
Vaginal progesterone is as effective as cervical cerclage to prevent preterm birth in women with a singleton gestation, previous spontaneous preterm birth, and a short cervix: updated indirect comparison meta-analysis.Am J Obstet Gynecol. 2018 Jul;219(1):10-25. doi: 10.1016/j.ajog.2018.03.028. Epub 2018 Apr 7. Am J Obstet Gynecol. 2018. PMID: 29630885 Free PMC article.
-
Vaginal progesterone to prevent preterm birth in pregnant women with a sonographic short cervix: clinical and public health implications.Am J Obstet Gynecol. 2016 Feb;214(2):235-242. doi: 10.1016/j.ajog.2015.09.102. Epub 2015 Oct 9. Am J Obstet Gynecol. 2016. PMID: 26450404 Free PMC article.
-
Cervical cerclage for singleton pregnant patients on vaginal progesterone with progressive cervical shortening.Am J Obstet Gynecol. 2018 Oct;219(4):397.e1-397.e10. doi: 10.1016/j.ajog.2018.06.020. Epub 2018 Jul 11. Am J Obstet Gynecol. 2018. PMID: 30017683
-
SMFM Consult Series #70: Management of short cervix in individuals without a history of spontaneous preterm birth.Am J Obstet Gynecol. 2024 Aug;231(2):B2-B13. doi: 10.1016/j.ajog.2024.05.006. Epub 2024 May 15. Am J Obstet Gynecol. 2024. PMID: 38754603
Cited by
-
Infection and smoking are associated with decreased plasma concentration of the anti-aging protein, α-klotho.J Perinat Med. 2013 Sep 1;41(5):581-94. doi: 10.1515/jpm-2013-0084. J Perinat Med. 2013. PMID: 23770558 Free PMC article.
-
Progesterone to prevent spontaneous preterm birth.Semin Fetal Neonatal Med. 2014 Feb;19(1):15-26. doi: 10.1016/j.siny.2013.10.004. Epub 2013 Dec 5. Semin Fetal Neonatal Med. 2014. PMID: 24315687 Free PMC article. Review.
-
Vaginal progesterone for preventing preterm birth and adverse perinatal outcomes in singleton gestations with a short cervix: a meta-analysis of individual patient data.Am J Obstet Gynecol. 2018 Feb;218(2):161-180. doi: 10.1016/j.ajog.2017.11.576. Epub 2017 Nov 17. Am J Obstet Gynecol. 2018. PMID: 29157866 Free PMC article.
-
The Maternal Serological Response to Intrauterine Ureaplasma sp. Infection and Prediction of Risk of Pre-Term Birth.Front Immunol. 2014 Dec 9;5:624. doi: 10.3389/fimmu.2014.00624. eCollection 2014. Front Immunol. 2014. PMID: 25538708 Free PMC article. Review.
-
17-alpha Hydroxyprogesterone caproate did not reduce the rate of recurrent preterm birth in a prospective cohort study.Am J Obstet Gynecol. 2017 Jun;216(6):600.e1-600.e9. doi: 10.1016/j.ajog.2017.02.025. Epub 2017 Feb 20. Am J Obstet Gynecol. 2017. PMID: 28223163 Free PMC article.
References
-
- Saling E. Prevention of prematurity - a complex undertaking reply. J Perinat Med. 2012;40:103. - PubMed
-
- Campbell S. Universal cervical-length screening and vaginal progesterone prevents early preterm births, reduces neonatal morbidity and is cost saving: doing nothing is no longer an option. Ultrasound in obstetrics & gynecology : the official journal of the International Society of Ultrasound in Obstetrics and Gynecology. 2011;38:1–9. - PubMed
-
- Romero R, Mazor M, Munoz H, Gomez R, Galasso M, Sherer DM. The preterm labor syndrome. Ann N Y Acad Sci. 1994;734:414–429. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources