

Case Reports
doi: 10.1136/bcr-2012-007055.
Anaphylaxis in pregnancy: a rare cause of neonatal mortality
Affiliations
- PMID: 23314874
- PMCID: PMC3603634
- DOI: 10.1136/bcr-2012-007055
Item in Clipboard
Case Reports
Anaphylaxis in pregnancy: a rare cause of neonatal mortality
BMJ Case Rep.
.
Abstract
Anaphylaxis is a rare condition in pregnancy. Drugs are the aetiological agents most often implicated. Maternal anaphylaxis can lead to significant fetal morbidity and even mortality if uterine perfusion and maternal oxygenation are compromised. Significant risk of neonatal neurological damage or death can occur even when the maternal clinical outcome is favourable. The authors present the case of a newborn, born at gestational age of 29 weeks, who died at 11 days of life with hypoxic-ischaemic cerebral injuries as a consequence of maternal anaphylaxis following the administration of amoxicillin in the community setting.
Figures
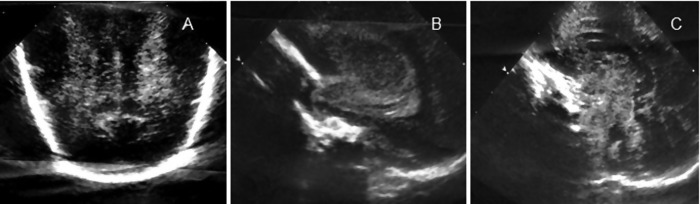
Cranial ultrasound. Coronal planes (A) and sagittal planes (B and C): symmetric, diffuse periventricular white matter echogenicity (A), hyperechoic aspect of cerebellum, thalami and basal ganglia (B and C).

MRI performed at 10 days of life: axial T1-weighted MRI showing frontoparietal, pericentral and temporal necrosis. Hypersignal of thalami and lentiform nuclei. Cavitation necrosis in brain stem—lesions compatible with diffuse hypoxic encephalomalacia.

Umbilical cord pathology. Presence of three umbilical vessels with severe vasoconstriction of umbilical arteries (arrow).

Placenta pathology. Placenta normal maturation. Mastocytes colouration was negative.

Newborn autopsy. Coronal plane of brain with the presence of subcortical leukomalacia (arrow).

Newborn autopsy. Thalami with an infarct lesion.

Newborn autopsy. Signs of neuronal necrosis at medulla oblongata—eosinophilic cytoplasm and pycnotic nuclei (arrow).
References
-
- Mulla ZD, Ebrahim MS, Gonzalez JL. Anaphylaxis in the obstetric patient: analysis of a statewide hospital discharge database. Ann Allergy Asthma Immunol 2010;104:55–9 - PubMed
-
- Chaudhuri K, Gonzales J, Jesurun CA, et al. Anaphylactic shock in pregnancy: a case study and review of the literature. Int J Obstet Anesth 2008;17:350–7 - PubMed
-
- Sengupta A, Kohli JK. Antibiotic prophylaxis in cesarean section causing anaphylaxis and intrauterine fetal death. J Obstet Gynaecol Res 2008;34:252–4 - PubMed
-
- Khan R, Anastasakis E, Kadir RA. Anaphylactic reaction to ceftriaxone in labour. An emerging complication. J Obstet Gynaecol 2008;28:751–3 - PubMed
-
- Gei AF, Pacheco LD, Vanhook JW, et al. The use of a continuous infusion of epinephrine for anaphylactic shock during labor. Obstet Gynecol 2003;102:1332–5 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical