

Health economic evaluation of the Lund Integrated Medicines Management Model (LIMM) in elderly patients admitted to hospital
- PMID: 23315436
- PMCID: PMC3553390
- DOI: 10.1136/bmjopen-2012-001563
Health economic evaluation of the Lund Integrated Medicines Management Model (LIMM) in elderly patients admitted to hospital
Abstract
Objective: To evaluate the cost effectiveness of a multidisciplinary team including a pharmacist for systematic medication review and reconciliation from admission to discharge at hospital among elderly patients (the Lund Integrated Medicines Management (LIMM)) in order to reduce drug-related readmissions and outpatient visits.
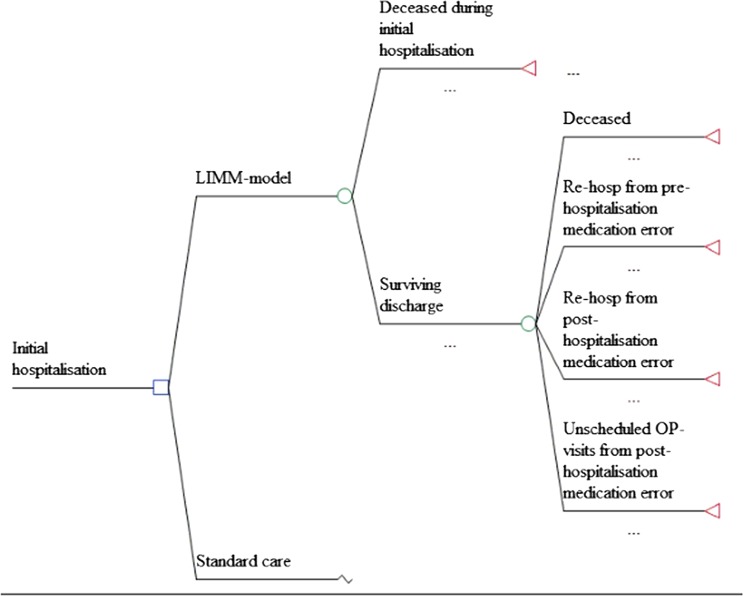
Method: Published data from the LIMM project group were used to design a probabilistic decision tree model for evaluating tools for (1) a systematic medication reconciliation and review process at initial hospital admission and during stay (admission part) and (2) a medication report for patients discharged from hospital to primary care (discharge part). The comparator was standard care. Inpatient, outpatient and staff time costs (Euros, 2009) were calculated during a 3-month period. Dis-utilities for hospital readmissions and outpatient visits due to medication errors were taken from the literature.
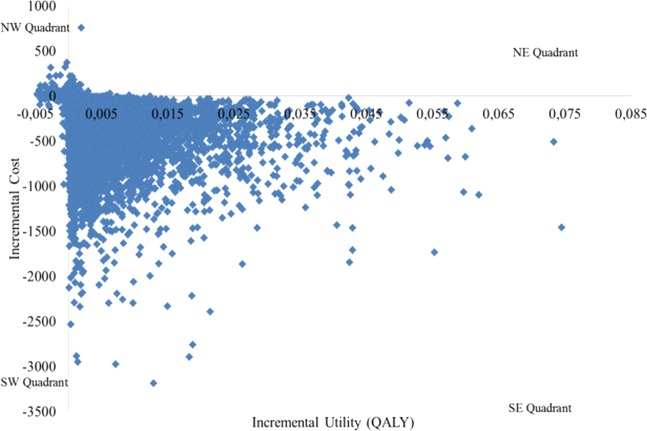
Results: The total cost for the LIMM model was €290 compared to €630 for standard care, in spite of a €39 intervention cost. The main cost offset arose from avoided drug-related readmissions in the Admission part (€262) whereas only €66 was offset in the Discharge part as a result of fewer outpatient visits and correction time. The reduced disutility was estimated to 0.005 quality-adjusted life-years (QALY), indicating that LIMM was a dominant alternative. The probability that the intervention would be cost-effective at a zero willingness to pay for a gained QALY compared to standard care was estimated to 98%.
Conclusions: The LIMM medication reconciliation (at admission and discharge) and medication review was both cost-saving and generated greater utility compared to standard care, foremost owing to avoided drug-related hospital readmissions. When implementing such a review process with a multidisciplinary team, it may be important to consider a learning curve in order to capture the full advantage.
Figures
References
-
- Institute for Healthcare Improvement Prevent adverse drug event with medication reconciliation. In: http://www.ihi.org/explore/ADEsMedicationReconciliation/Pages/default.aspx (accessed 6 Jan 2013).
-
- Lazarou J, Pomeranz BH, Corey PN. Incidence of adverse drug reactions in hospitalized patients: a meta-analysis of prospective studies (see comments). JAMA 1998;279:1200–5 - PubMed
-
- Bootman JL, Harrison DL, Cox E. The health care cost of drug-related morbidity and mortality in nursing facilities. Arch Intern Med 1997;157:2089–96 - PubMed
-
- Beijer HJ, de Blaey CJ. Hospitalisations caused by adverse drug reactions (ADR): a meta-analysis of observational studies. Pharm World Sci 2002;24:46–54 - PubMed
-
- Hohl CM, Nosyk B, Kuramoto L, et al. Outcomes of emergency department patients presenting with adverse drug events. Ann Emerg Med 2011;58:270–9 - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources