

Acute right ventricular failure in a patient with hepatic cirrhosis
- PMID: 23316403
- PMCID: PMC3535729
- DOI: 10.1155/2012/127583
Acute right ventricular failure in a patient with hepatic cirrhosis
Abstract
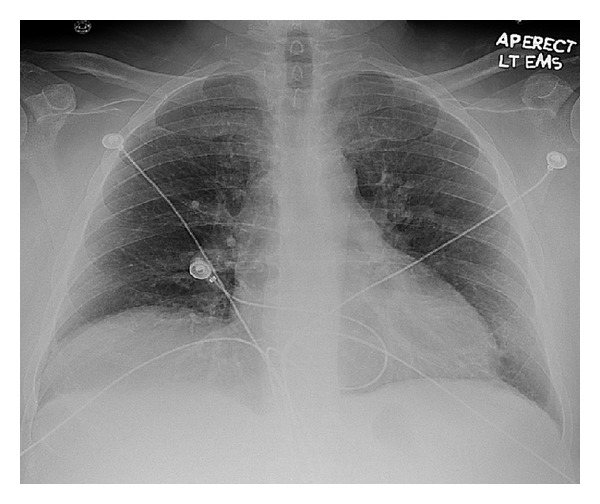
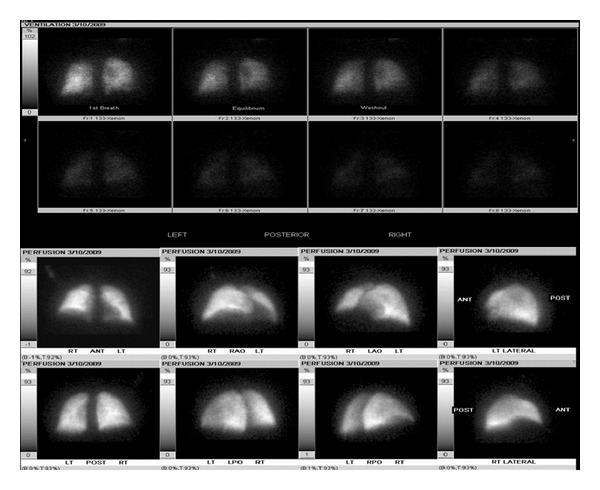
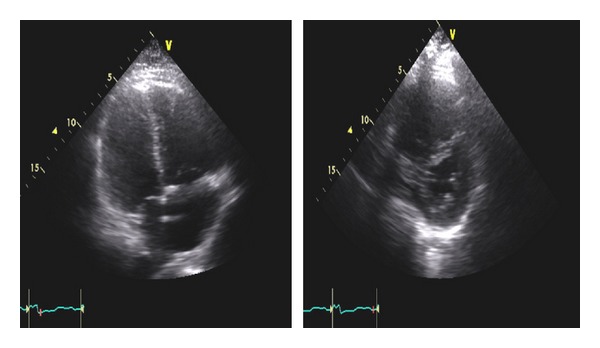
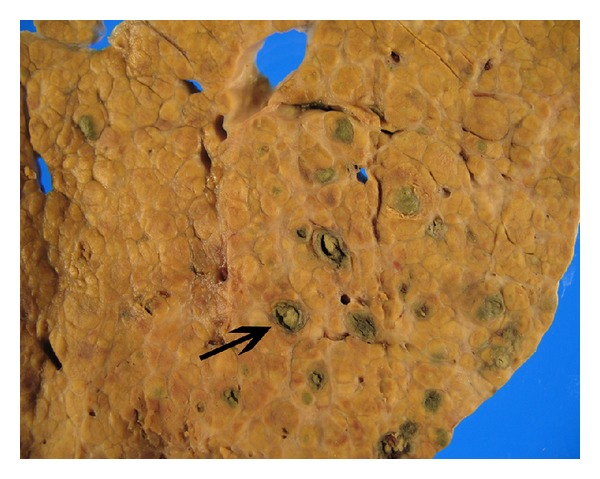
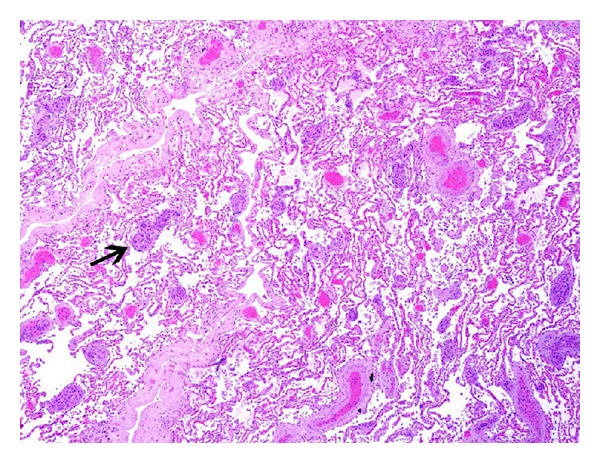
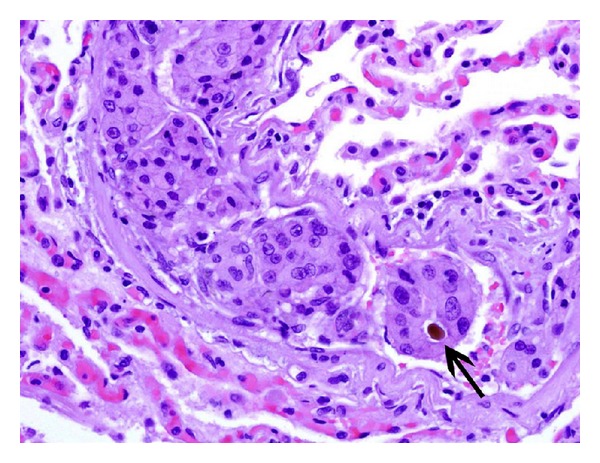
Pulmonary embolic disease is most commonly a manifestation of venous thromboembolism (VTE). However, fat, tumor, and air may all embolize to the pulmonary vasculature and lymphatics resulting in various clinical manifestations. Tumor emboli to small pulmonary vessels and lymphatics can lead to hypoxemic respiratory failure and shock. We present a 62-year-old male with history of mild COPD and end-stage liver disease secondary to hepatitis C admitted due to progressive shortness of breath and hypoxemia who developed shock and right ventricular failure. After a negative evaluation for venous thromboembolic disease, he had progressive respiratory and hemodynamic deterioration despite mechanical ventilation, renal replacement therapy, and vasopressive/inotropic support. Postmortem examination revealed diffuse micronodular moderately differentiated hepatocellular carcinoma (HCC) without a discrete mass, as well as numerous HCC tumor emboli to the lung and focally to the heart, consistent with disseminated hepatocellular tumor microembolism.
Figures
Similar articles
-
Hepatocellular Carcinoma With Tumor Thrombus to the Hepatic Veins and the Right Atrium: A Case Report and Review Exploring Various Presentations and Treatment Options.Cureus. 2020 Jun 2;12(6):e8405. doi: 10.7759/cureus.8405. Cureus. 2020. PMID: 32637284 Free PMC article.
-
[Right heart failure due to pulmonary tumor microembolism -- a rare differential diagnosis].Pneumologie. 2004 Jun;58(6):400-3. doi: 10.1055/s-2004-818458. Pneumologie. 2004. PMID: 15216432 German.
-
Intravascular B-cell lymphoma: case report of a rare cause of pulmonary arterial hypertension.Eur Heart J Case Rep. 2019 Feb 2;3(1):yty150. doi: 10.1093/ehjcr/yty150. eCollection 2019 Mar. Eur Heart J Case Rep. 2019. PMID: 31020226 Free PMC article.
-
Massive pulmonary tumor microembolism from a hepatocellular carcinoma.Pathol Res Pract. 2006;202(5):395-9. doi: 10.1016/j.prp.2006.01.005. Epub 2006 Feb 20. Pathol Res Pract. 2006. PMID: 16488087 Review.
-
Refractory Hypoxemia in a Patient with Submassive Pulmonary Embolism and an Intracardiac Shunt: A Case Report and Review of the Literature.Perm J. 2018;22:17-061. doi: 10.7812/TPP/17-061. Perm J. 2018. PMID: 29616915 Free PMC article. Review.
Cited by
-
From the liver to the foot: a case of systemic embolism and acrometastasis in hepatocellular carcinoma.Gastrointest Cancer Res. 2014 May;7(3-4):103-7. Gastrointest Cancer Res. 2014. PMID: 25276264 Free PMC article. No abstract available.
References
-
- Spencer H. Pathology of the Lung. 3rd edition. Vol. 2. London, UK: Pergamon Press; 1977.
-
- Maza I, Braun E, Plotkin A, Guralnik L, Azzam ZS. Lymphangitis carcinomatosis of unknown origin presenting as severe pulmonary hypertension. American Journal of the Medical Sciences. 2004;327(5):255–257. - PubMed
-
- Kane RD, Hawkins HK, Miller JA, Noce PS. Microscopic pulmonary tumor emboli associated with dyspnea. Cancer. 1975;36(4):1473–1482. - PubMed
-
- Bruce DM, Keys SD, Eremin O. Lymphangitis carcinomatosa: a literature review. Journal of the Royal College of Surgeons of Edinburgh. 1996;41(1):7–13. - PubMed
-
- Sood N, Bandarenko N, Paradowski LJ. Case 2: acute respiratory failure secondary to lymphangitic carcinomatosis. Journal of Clinical Oncology. 2000;18(1):229–232. - PubMed
LinkOut - more resources
Full Text Sources
