

Pulmonary focal fibrosis associated with microscopic arterio-venous fistula manifesting as focal ground-glass opacity on thin-section CT
- PMID: 23316757
- PMCID: PMC3561274
- DOI: 10.1186/1471-2466-13-3
Pulmonary focal fibrosis associated with microscopic arterio-venous fistula manifesting as focal ground-glass opacity on thin-section CT
Abstract
Background: Focal ground-glass opacity (GGO) on thin-section computed tomography (CT) may be seen in atypical adenomatous hyperplasia (AAH), adenocarcinoma in situ that has recently been renamed from bronchioloalveolar carcinoma (BAC) and various benign conditions.
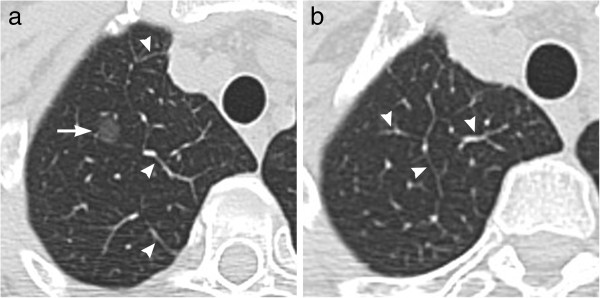
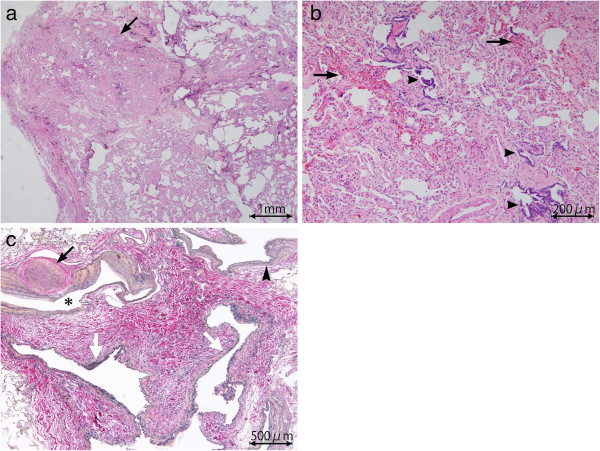
Case presentation: We report a case of pulmonary focal fibrosis associated with microscopic arterio-venous fistula (AVF), which showed a focal area of GGO on thin-section CT. The patient was a 58-year-old woman with a GGO on thin-section CT which had increased in size over the period of 2 years. Slightly dilated vessels and thickened interlobular septa were also noted around the GGO. It was diagnosed preoperatively as adenocarcinoma in situ and a partial lung resection by video-assisted thoracic surgery (VATS) was performed. Pathological examination yielded a diagnosis of focal fibrosis associated with microscopic AVF.
Conclusion: We speculate that the focal fibrosis was produced by a prolonged congestion due to the AVF and that the dilated vessels and thickening of interlobular septa on thin-section CT related to the AVF. Microscopic AVF may be one of the etiologies of focal fibrosis showing focal GGO on thins-section CT. Dilated vessels and thickened interlobular septa around the GGO might offer a clue to the diagnosis of this disease entity. In addition, it should be noted that focal fibrosis may increase in size.
Figures

References
-
- Travis WD, Brambilla E, Noguchi M, Nicholson AG, Geisinger KR, Yatabe Y, Beer DG, Powell CA, Riely GJ, Van Schil PE, Garg K, Austin JH, Asamura H, Rusch VW, Hirsch FR, Scagliotti G, Mitsudomi T, Huber RM, Ishikawa Y, Jett J, Sanchez-Cespedes M, Sculier JP, Takahashi T, Tsuboi M, Vansteenkiste J, Wistuba I, Yang PC, Aberle D, Brambilla C, Flieder D. et al. International association for the study of lung cancer/american thoracic society/european respiratory society international multidisciplinary classification of lung adenocarcinoma. J Thorac Oncol. 2011;6:244–285. doi: 10.1097/JTO.0b013e318206a221. - DOI - PMC - PubMed
-
- Collins J, Stern EJ. Ground-glass opacity at CT: The ABCs. AJR Am J Roentgenol. 1997;169:355–367. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
