

Absence of IL-1β positively affects neurological outcome, lesion development and axonal plasticity after spinal cord injury
- PMID: 23317037
- PMCID: PMC3585738
- DOI: 10.1186/1742-2094-10-6
Absence of IL-1β positively affects neurological outcome, lesion development and axonal plasticity after spinal cord injury
Abstract
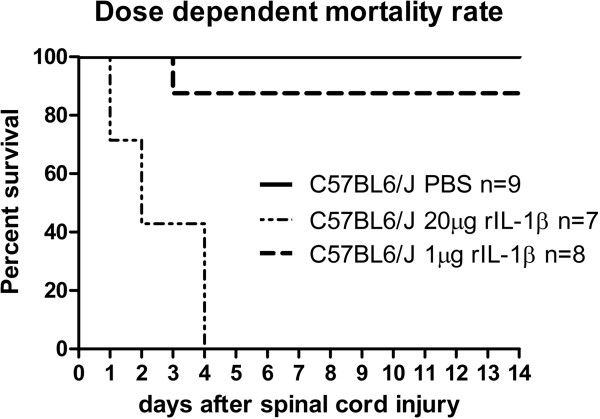
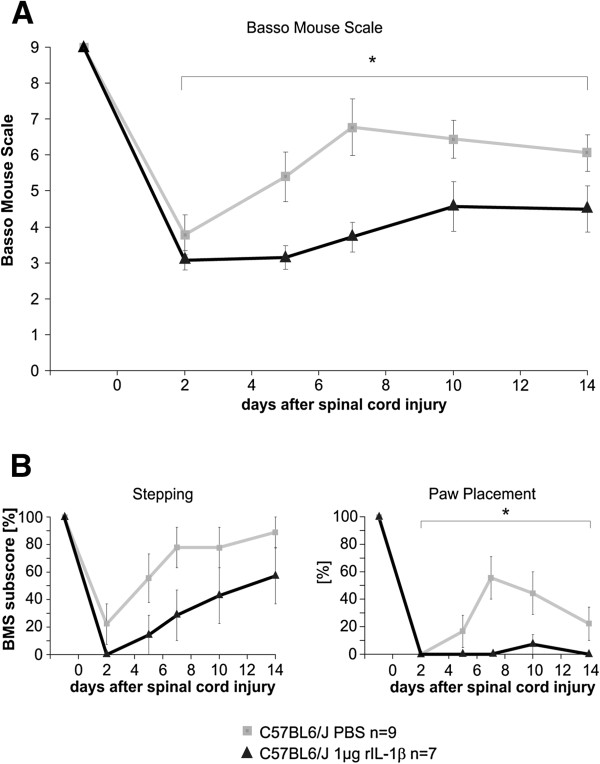
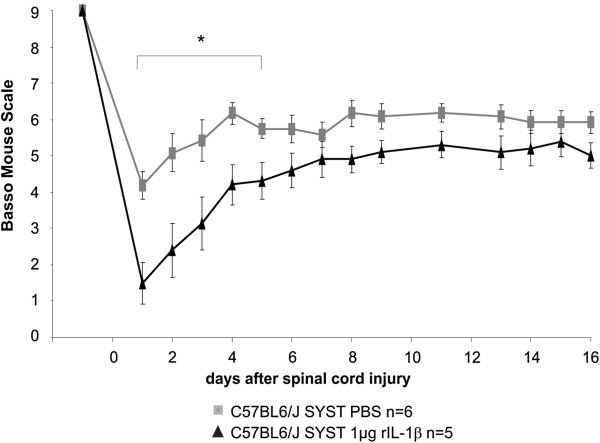
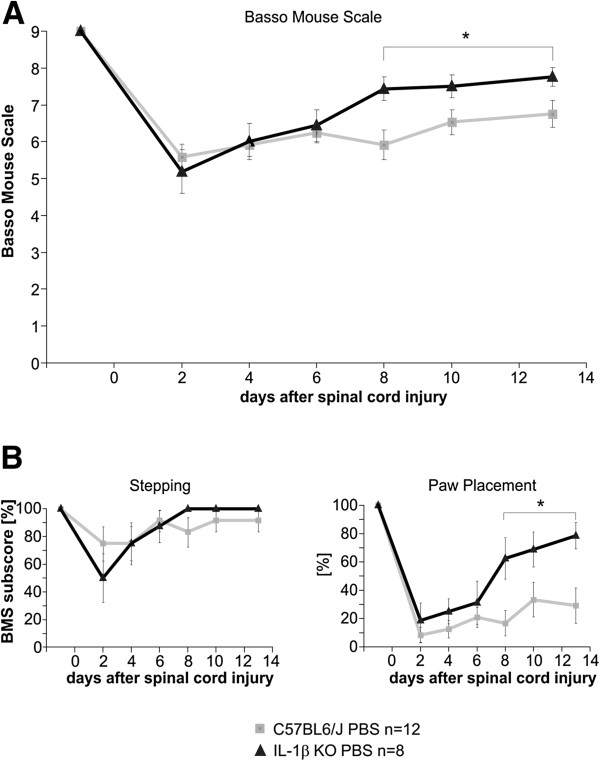
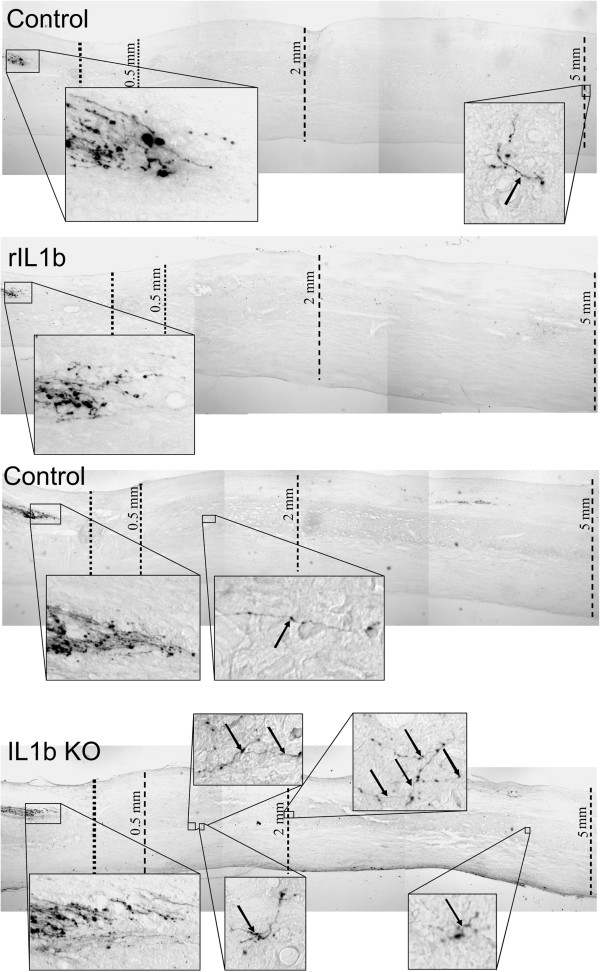
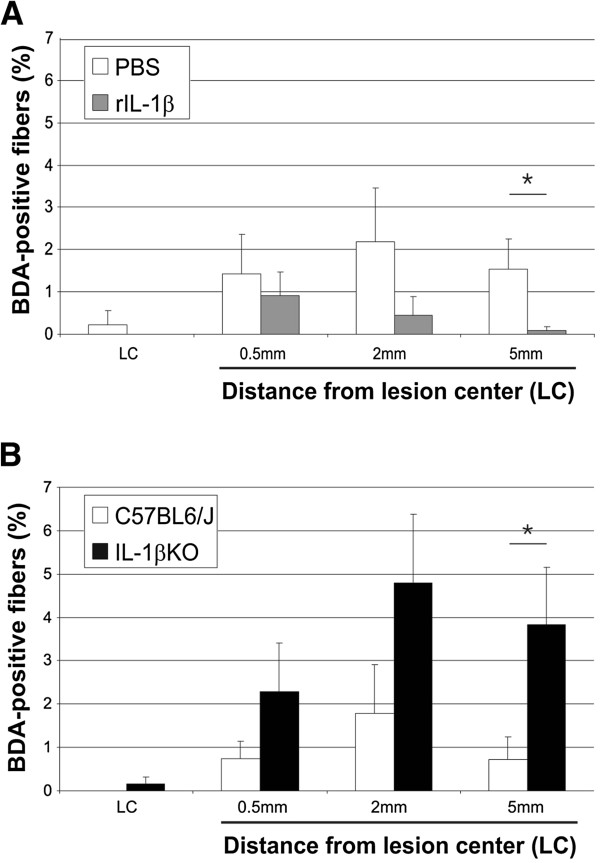
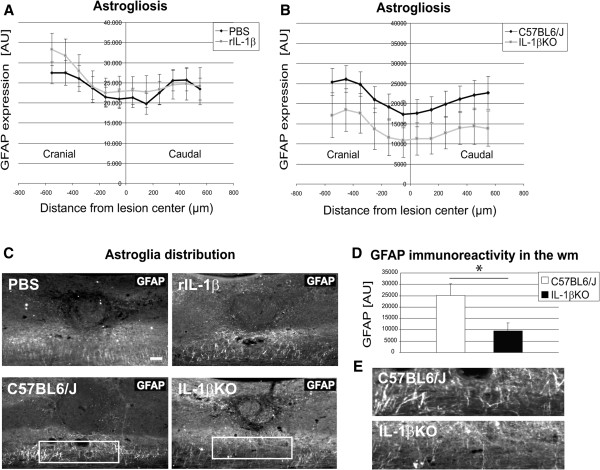
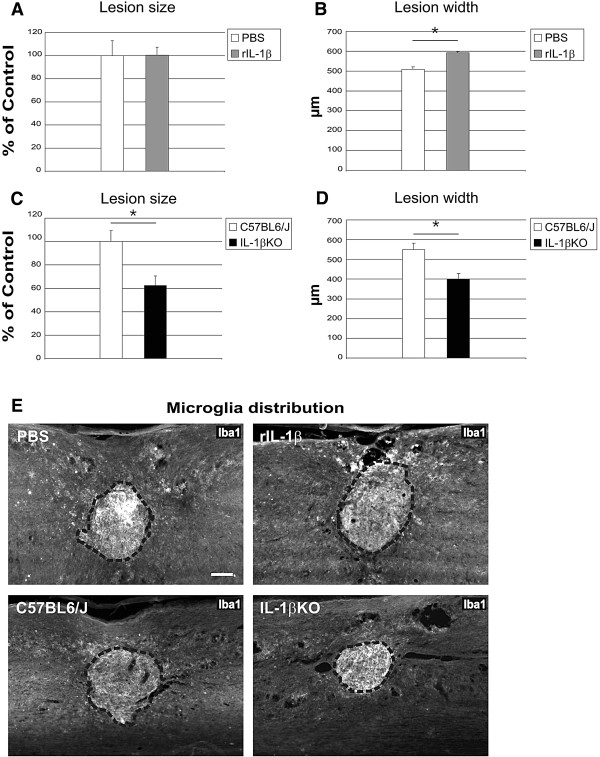
Precise crosstalk between the nervous and immune systems is important for neuroprotection and axon plasticity after injury. Recently, we demonstrated that IL-1β acts as a potent inducer of neurite outgrowth from organotypic brain slices in vitro, suggesting a potential function of IL-1β in axonal plasticity. Here, we have investigated the effects of IL-1β on axon plasticity during glial scar formation and on functional recovery in a mouse model of spinal cord compression injury (SCI). We used an IL-1β deficiency model (IL-1βKO mice) and administered recombinant IL-1β. In contrast to our hypothesis, the histological analysis revealed a significantly increased lesion width and a reduced number of corticospinal tract fibers caudal to the lesion center after local application of recombinant IL-1β. Consistently, the treatment significantly worsened the neurological outcome after SCI in mice compared with PBS controls. In contrast, the absence of IL-1β in IL-1βKO mice significantly improved recovery from SCI compared with wildtype mice. Histological analysis revealed a smaller lesion size, reduced lesion width and greatly decreased astrogliosis in the white matter, while the number of corticospinal tract fibers increased significantly 5 mm caudal to the lesion in IL-1βKO mice relative to controls. Our study for the first time characterizes the detrimental effects of IL-1β not only on lesion development (in terms of size and glia activation), but also on the plasticity of central nervous system axons after injury.
Figures
References
-
- Viviani B, Bartesaghi S, Gardoni F, Vezzani A, Behrens MM, Bartfai T, Binaglia M, Corsini E, Di Luca M, Galli CL, Marinovich M. Interleukin-1β enhances NMDA receptor-mediated intracellular calcium increase through activation of the Src family of kinases. J Neurosci. 2003;23:8692–8700. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
