

HIV-1 subtype distribution and its demographic determinants in newly diagnosed patients in Europe suggest highly compartmentalized epidemics
- PMID: 23317093
- PMCID: PMC3564855
- DOI: 10.1186/1742-4690-10-7
HIV-1 subtype distribution and its demographic determinants in newly diagnosed patients in Europe suggest highly compartmentalized epidemics
Abstract
Background: Understanding HIV-1 subtype distribution and epidemiology can assist preventive measures and clinical decisions. Sequence variation may affect antiviral drug resistance development, disease progression, evolutionary rates and transmission routes.
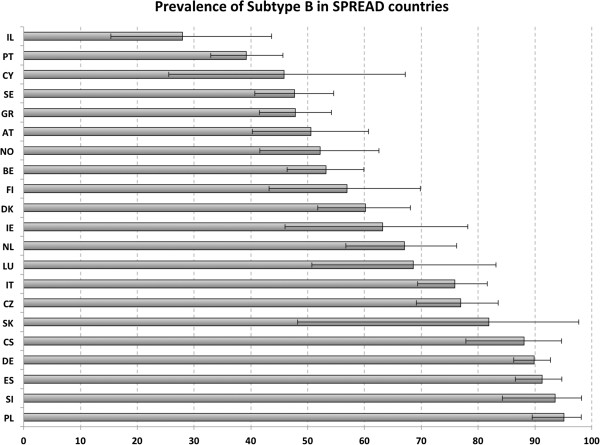
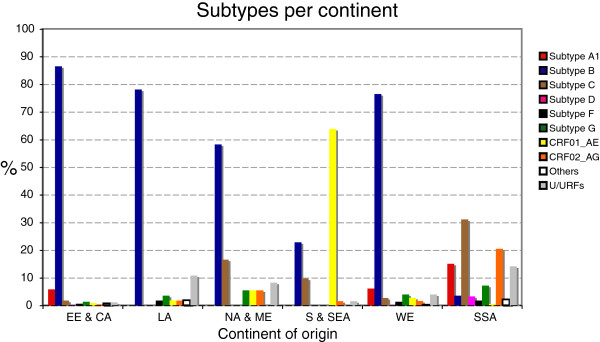
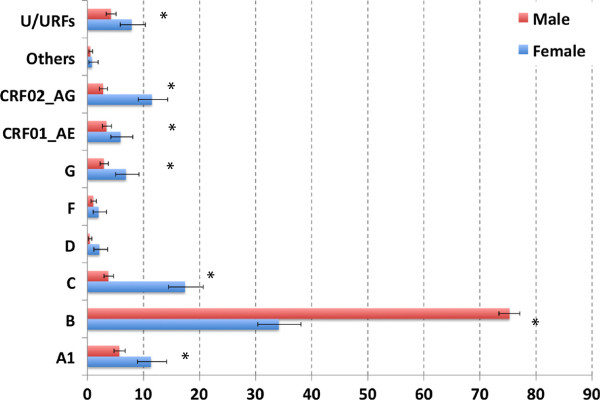
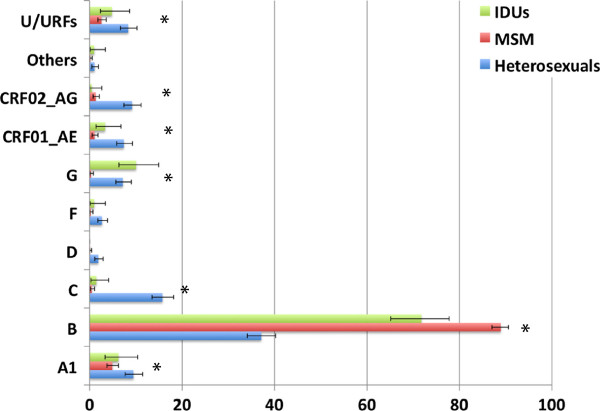
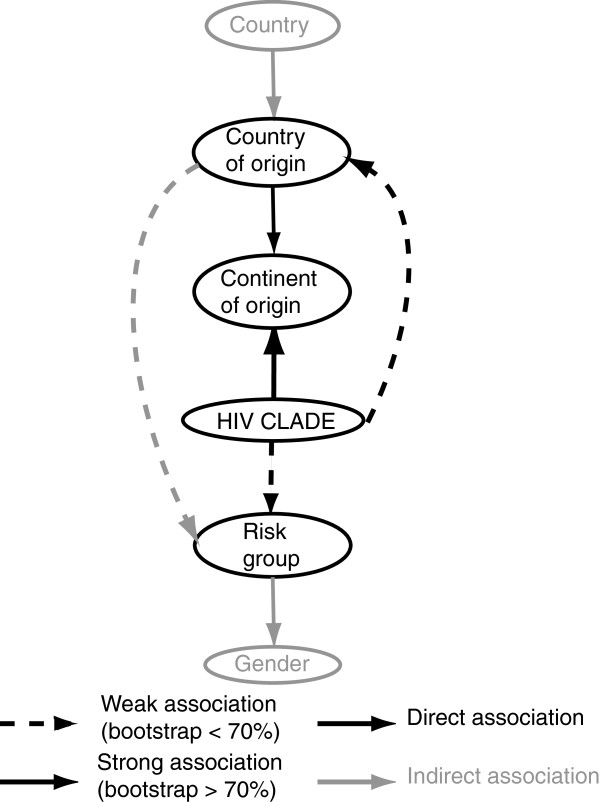
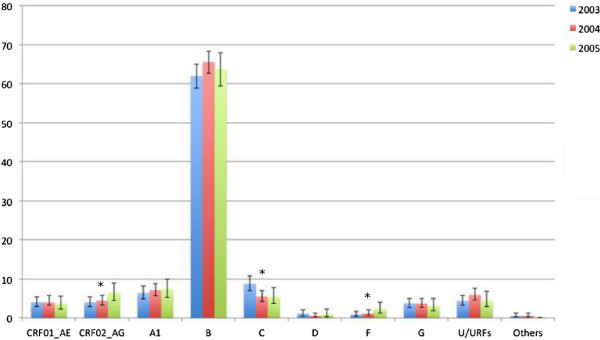
Results: We investigated the subtype distribution of HIV-1 in Europe and Israel in a representative sample of patients diagnosed between 2002 and 2005 and related it to the demographic data available. 2793 PRO-RT sequences were subtyped either with the REGA Subtyping tool or by a manual procedure that included phylogenetic tree and recombination analysis. The most prevalent subtypes/CRFs in our dataset were subtype B (66.1%), followed by sub-subtype A1 (6.9%), subtype C (6.8%) and CRF02_AG (4.7%). Substantial differences in the proportion of new diagnoses with distinct subtypes were found between European countries: the lowest proportion of subtype B was found in Israel (27.9%) and Portugal (39.2%), while the highest was observed in Poland (96.2%) and Slovenia (93.6%). Other subtypes were significantly more diagnosed in immigrant populations. Subtype B was significantly more diagnosed in men than in women and in MSM > IDUs > heterosexuals. Furthermore, the subtype distribution according to continent of origin of the patients suggests they acquired their infection there or in Europe from compatriots.
Conclusions: The association of subtype with demographic parameters suggests highly compartmentalized epidemics, determined by social and behavioural characteristics of the patients.
Figures
References
-
- Robertson DL, Anderson JP, Bradac JA, Carr JK, Foley B, Funkhouser RK, Gao F, Hahn BH, Kalish ML, Kuiken C. et al. HIV-1 nomenclature proposal. Science. 2000;288:55–55. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
