

Impact of rectal balloon-filling materials on the dosimetry of prostate and organs at risk in photon beam therapy
- PMID: 23318385
- PMCID: PMC5713667
- DOI: 10.1120/jacmp.v14i1.3993
Impact of rectal balloon-filling materials on the dosimetry of prostate and organs at risk in photon beam therapy
Abstract
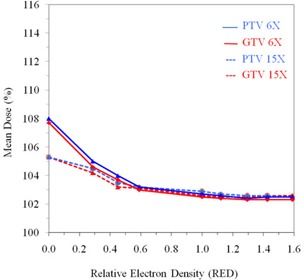
The use of rectal balloon in radiotherapy of prostate cancer is shown to be effective in reducing prostate motion and minimizing rectal volume, thus reducing rectal toxicity. Air-filled rectal balloon has been used most commonly, but creates dose perturbation at the air-tissue interface. In this study, we evaluate the effects of rectal balloon-filling materials on the dose distribution to the target and organs at risk. The dosimetric impact of rectal balloon filling was studied in detail for a typical prostate patient, and the general effect of the balloon filling was investigated from a study of ten prostate patients covering a wide range of anterior-posterior and left-right separations, as well as rectal and bladder volumes. Hounsfield units (HU) of the rectal balloon filling was changed from -1000 HU to 1000 HU at an interval of 250 HU, and the corresponding changes in the relative electron density (RED) was calculated. For each of the HU of the rectal balloon filling, a seven-field IMRT plan was generated with 6 MV and 15 MV photon beams, respectively. Dosimetric evaluation was performed with the AAA algorithm for inhomogeneity corrections. A detailed study of the rectal balloon filling shows that the GTV, PTV, rectal, and bladder mean dose decreased with increasing values of RED in the rectal balloon. There is significant underdosage in the target volume at the rectum-prostate interface with an air-filled balloon as compared to that with a water-filled balloon for both 6 MV and 15 MV beams. While the dosimetric effect of the rectal balloon filling is reduced when averaged over ten patients, generally an air-filled balloon results in lower minimum dose and lower mean dose in the overlap region (and possibly the PTV) compared to those produced by water-filled or contrast-filled balloons. Dose inhomogeneity in the target volume is increased with an air-filled rectal balloon. Thus a water-filled or contrast-filled rectal balloon is preferred to an air-filled rectal balloon in EBRT of prostate treatment.
Figures





Similar articles
-
Rectal wall sparing by dosimetric effect of rectal balloon used during intensity-modulated radiation therapy (IMRT) for prostate cancer.Med Dosim. 2005 Spring;30(1):25-30. doi: 10.1016/j.meddos.2004.10.005. Med Dosim. 2005. PMID: 15749008
-
The use of rectal balloon during the delivery of intensity modulated radiotherapy (IMRT) for prostate cancer: more than just a prostate gland immobilization device?Cancer J. 2002 Nov-Dec;8(6):476-83. doi: 10.1097/00130404-200211000-00012. Cancer J. 2002. PMID: 12500857
-
Rectal dose sparing with a balloon catheter and ultrasound localization in conformal radiation therapy for prostate cancer.Radiother Oncol. 2003 Jun;67(3):285-94. doi: 10.1016/s0167-8140(03)00056-2. Radiother Oncol. 2003. PMID: 12865176
-
The use of spatial dose gradients and probability density function to evaluate the effect of internal organ motion for prostate IMRT treatment planning.Phys Med Biol. 2007 Mar 7;52(5):1469-84. doi: 10.1088/0031-9155/52/5/016. Epub 2007 Feb 12. Phys Med Biol. 2007. PMID: 17301465
-
The influence of a rectal balloon tube as internal immobilization device on variations of volumes and dose-volume histograms during treatment course of conformal radiotherapy for prostate cancer.Int J Radiat Oncol Biol Phys. 2002 Jan 1;52(1):91-100. doi: 10.1016/s0360-3016(01)01821-1. Int J Radiat Oncol Biol Phys. 2002. PMID: 11777626
References
-
- Ten Haken RK, Forman JD, Heimburger DK, et al. Treatment planning issues related to prostate movement in response to differential filling of the rectum and bladder. Int J Radiat Oncol Biol Phys. 1991;20(6):1317–24. - PubMed
-
- Dunscombe P, Loose S, Leszczynski K. Sizes and sources of field placement error in routine irradiation for prostate cancer. Radiother Oncol. 1993;26(2):174–76. - PubMed
-
- Roeske JC, Forman JD, Mesina CF, et al. Evaluation of changes in the size and location of the prostate, seminal vesicles, bladder, and rectum during a course of external beam radiation therapy. Int J Radiat Oncol Biol Phys. 1995;33(5):1321–29. - PubMed
-
- Balter JM, Lam KL, Sandler HM, Littles JF, Bree RL, Ten Haken RK. Automated localization of the prostate at the time of treatment using implanted radiopaque markers: technical feasibility. Int J Radiat Oncol Biol Phys. 1995;33(5):1281–86. - PubMed
-
- van Herk M, Bruce A, Kroes AP, Shouman T, Touw A, Lebesque JV. Quantification of organ motion during conformal radiotherapy of the prostate by three dimensional image registration. Int J Radiat Oncol Biol Phys. 1995;33(5):1311–20. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
