

Effectiveness of disseminating consensus management recommendations for ulcer bleeding: a cluster randomized trial
- PMID: 23318399
- PMCID: PMC3576461
- DOI: 10.1503/cmaj.120095
Effectiveness of disseminating consensus management recommendations for ulcer bleeding: a cluster randomized trial
Abstract
Background: International guidelines for the management of nonvariceal upper gastrointestinal bleeding have not been widely adopted in clinical practice. We sought to determine whether a national, multifaceted intervention could improve adherence to guidelines, especially for patients at high risk of nonvariceal upper gastrointestinal bleeding.
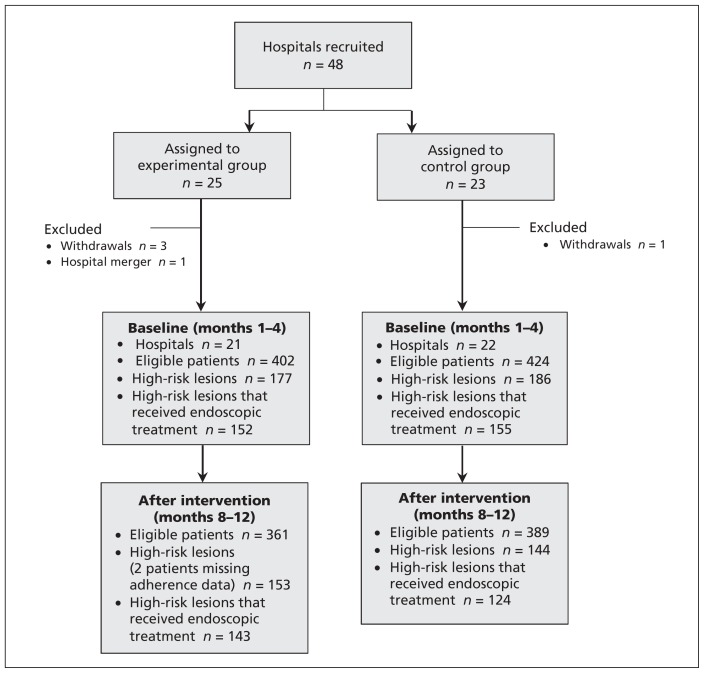
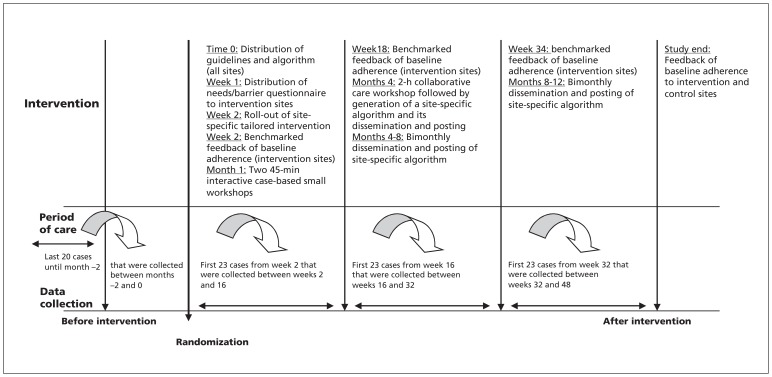
Methods: In this randomized trial, we stratified hospitals by region and size and allocated sites to either the control or experimental group. Health care workers in the experimental group were given published guidelines, generic algorithms, stratification scoring systems and written reminders and attended multidisciplinary guideline education groups and case-based workshops. These interventions were implemented over a 12-month period after randomization, with performance feedback and benchmarking. The primary outcome of adherence rates to key guidelines in endoscopic and pharmacologic management, determined by chart review, was adjusted according to site characteristics and possible within-site dependencies. We also report the rates of adherence to other recommendations.
Results: Forty-three sites were randomized to the experimental (n=21) or control (n=22) groups. In our primary analysis, we compared patients before (experimental group: n=402 patients; control group: n=424 patients) and after (experimental group: n=361 patients; control group: n=389 patients) intervention. Patient-level analysis revealed no significant difference in adherence rates to the guidelines after the intervention (experimental group: 9.8%; control group: 4.8%; p=0.99) after adjustment for the rate of adherence before the intervention (experimental group: 13.2%; control group: 7.1%). The adherence rates to other guidelines were similar and decreased over time, varying between 5% and 93%.
Interpretation: This national knowledge translation-based trial suggests poor adherence to guidelines on nonvariceal upper gastrointestinal bleeding. Adherence was not improved by an educational intervention, which highlights both the complexity and poor predictability of attempting to alter the behaviour of health care providers (Trial registration: ClinicalTrials.gov, no. MCT-88113).
Trial registration: ClinicalTrials.gov NCT00840008.
Figures
References
-
- Barkun A, Bardou M, Marshall JK. Consensus recommendations for managing patients with nonvariceal upper gastrointestinal bleeding. Ann Intern Med 2003;139:843–57 - PubMed
-
- Bensoussan K, Fallone CA, Barkun AN, et al. A sampling of Canadian practice in managing nonvariceal upper gastrointestinal bleeding before recent guideline publication: Is there room for improvement? Can J Gastroenterol 2005;19:487–95 - PubMed
-
- Marmo R, Koch M, Cipolletta L, et al. Predictive factors of mortality from nonvariceal upper gastrointestinal hemorrhage: a multicenter study. Am J Gastroenterol 2008;103:1639–47, quiz 48. - PubMed
-
- Barkun A, Gasco A, Jewell D, et al. ; REASON Study Investigators Management of Nonvariceal Upper GI Bleeding (NVUGIB) after guideline publication: the REASON study. Can J Gastro. 2006;20(suppl A):80A
-
- Barkun A, Enns R, Romagnuolo J, et al. The Drug Utilization Review of Acid suppressants for BLEeding and other indications (DURABLE) — a national audit to assess the current utilization of proton pump inhibitors and histamine H2-receptor antagonists in Canadian hospitals [abstract]. Am J Gastroenterol 2007; 102:S173
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical