

Defective barrier function in neosquamous epithelium
- PMID: 23318477
- PMCID: PMC3838860
- DOI: 10.1038/ajg.2012.440
Defective barrier function in neosquamous epithelium
Abstract
Objectives: Radiofrequency ablation (RFA) of Barrett's esophagus (BE) is a common strategy for the prevention of esophageal adenocarcinoma (EAC). After RFA, the ablated esophagus heals on acid suppressive therapy, and is re-populated with a stratified squamous epithelium, referred to as "neosquamous epithelium (NSE)." Because the ability of the NSE to protect the underlying tissue from recurrent insult by reflux is unclear, we assessed the barrier function of NSE by comparing it to that of the native upper squamous epithelium (USE) in subjects having undergone RFA.
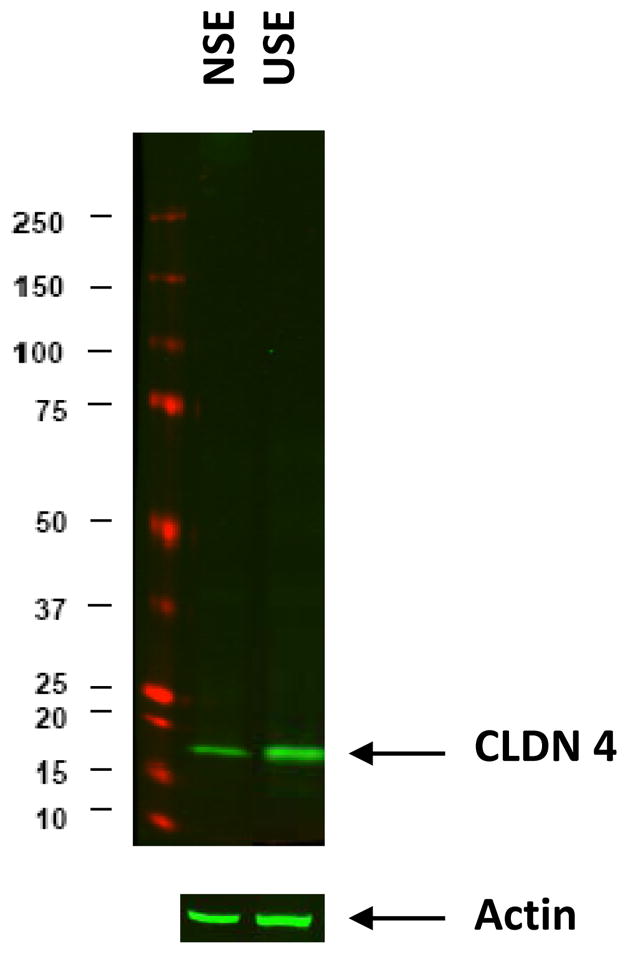
Methods: At varying intervals following RFA, the barrier function of NSE and USE were assessed in endoscopic biopsies by light and electron microscopy, and by measurement of electrical resistance (R) and fluorescein flux in mini-Ussing chambers. Chamber results were further compared with results from control biopsies (healthy distal esophagus). A claudin expression profile in the tight junctions (TJs) of NSE and USE was determined using Quantitative reverse transcriptase PCR. Differential expression of claudin-4 between NSE and USE was assayed by immunoblots.
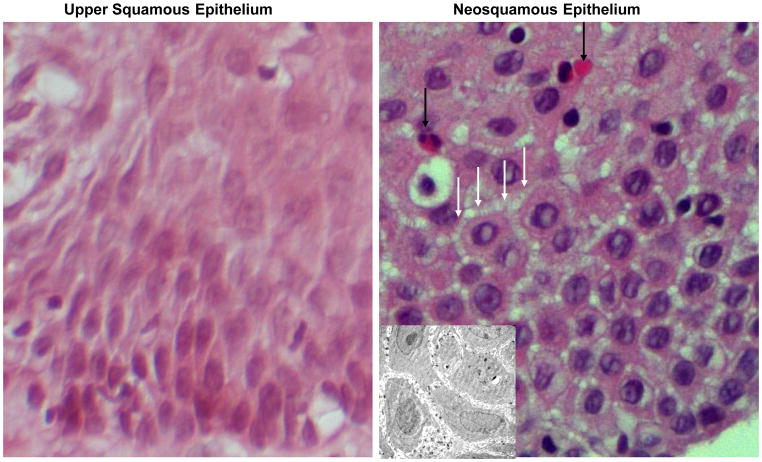
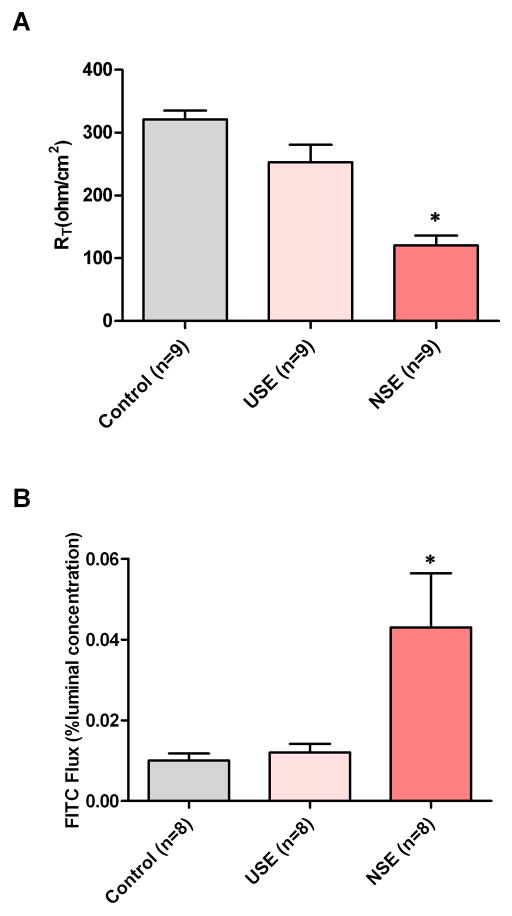
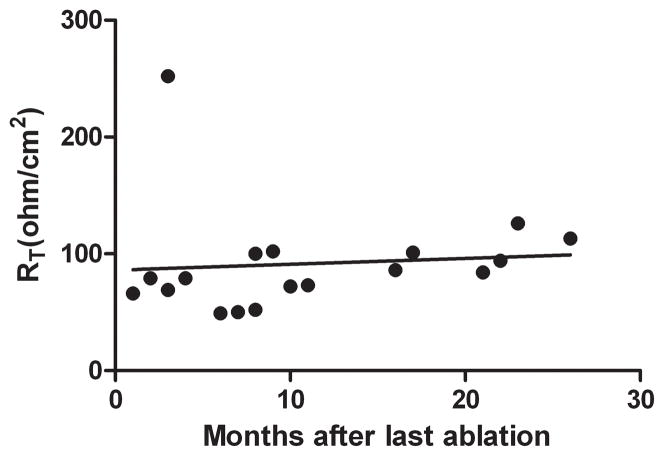
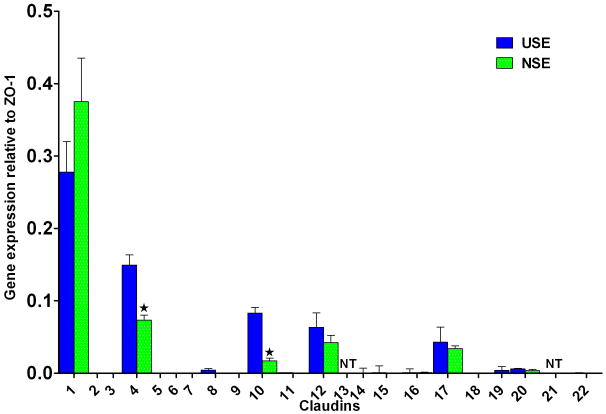
Results: USE was histologically normal whereas NSE showed dilated intercellular spaces and marked eosinophilia. NSE was also more permeable than USE and healthy controls, having lower mean R and higher fluorescein fluxes. Abnormally low R values for NSE were unrelated to the time period following RFA (or number of prior RFA sessions), being abnormal even 26 months after RFA. Abnormal permeability in NSE was associated with significantly lower values for claudin-4 and claudin-10 than in USE.
Conclusions: NSE commonly exhibits defective barrier function. As this defect will make it vulnerable to injury, inflammation, and destruction by acidic and weakly acidic refluxates, it may in part explain incidences of recurrence of BE following ablation.
Figures
References
-
- Shaheen NJ, Richter JE. Barrett’s oesophagus. Lancet. 2009;373(9666):850–61. - PubMed
-
- Spechler SJ. Barrett’s esophagus. In: Orlando RC, editor. Gastroesophageal Reflux Disease. New York: Marcel Dekker, Inc; 2000. pp. 219–258.
-
- Orlando RC. Mucosal Defense in Barrett’s Esophagus. In: Sharma P, Sampliner R, editors. Barrett’s Esophagus and Esophageal Adenocarcinoma. 2. Blackwell Publishing, Ltd; Oxford, UK: 2006. pp. 60–72.
-
- Jovov B, Van Itallie CM, Shaheen NJ, Carson JL, Gambling TM, Anderson JM, Orlando RC. Claudin-18: A Dominant Tight Junction Protein in Barrett’s Esophagus and Likely Contributor to its Acid Resistance. Am J Physiol Gastrointest Liver Physiol. 2007;293(6):G1106–13. - PubMed
-
- Hvid-Jensen F, Pedersen L, Drewes AM, Sørensen HT, Funch-Jensen P. Incidence of adenocarcinoma among patients with Barrett’s esophagus. N Engl J Med. 2011;365(15):1375–83. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
