

A tale of two cities: the role of neighborhood socioeconomic status in spatial clustering of bystander CPR in Austin and Houston
- PMID: 23318916
- PMCID: PMC3762246
- DOI: 10.1016/j.resuscitation.2013.01.007
A tale of two cities: the role of neighborhood socioeconomic status in spatial clustering of bystander CPR in Austin and Houston
Abstract
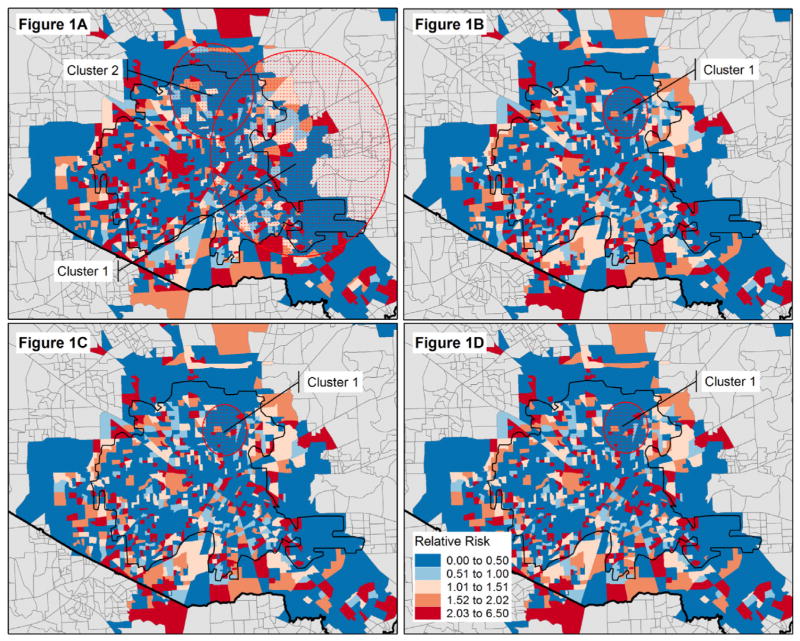
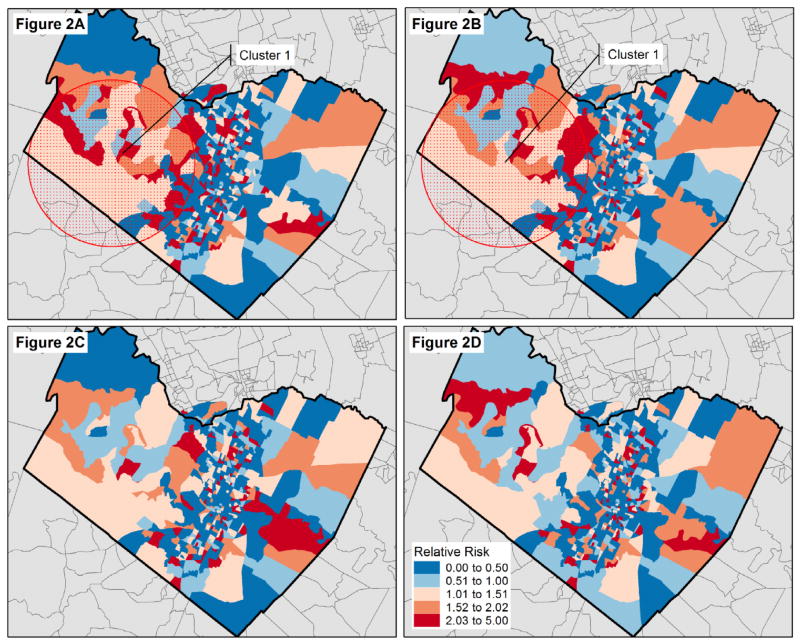
Background: Despite evidence to suggest significant spatial variation in out-of-hospital cardiac arrest (OHCA) and bystander cardiopulmonary resuscitation (BCPR) rates, geographic information systems (GIS) and spatial analysis have not been widely used to understand the reasons behind this variation. This study employs spatial statistics to identify the location and extent of clusters of bystander CPR in Houston and Travis County, TX.
Methods: Data were extracted from the Cardiac Arrest Registry to Enhance Survival for two U.S. sites - Austin-Travis County EMS and the Houston Fire Department - between October 1, 2006 and December 31, 2009. Hierarchical logistic regression models were used to assess the relationship between income and racial/ethnic composition of a neighborhood and BCPR for OHCA and to adjust expected counts of BCPR for spatial cluster analysis. The spatial scan statistic was used to find the geographic extent of clusters of high and low BCPR.
Results: Results indicate spatial clusters of lower than expected BCPR rates in Houston. Compared to BCPR rates in the rest of the community, there was a circular area of 4.2km radius where BCPR rates were lower than expected (RR=0.62; p<0.0001 and RR=0.55; p=0.037) which persist when adjusted for individual-level patient characteristics (RR=0.34; p=0.027) and neighborhood-level race (RR=0.34; p=0.034) and household income (RR=0.34; p=0.046). We also find a spatial cluster of higher than expected BCPR in Austin. Compared to the rest of the community, there was a 23.8km radius area where BCPR rates were higher than expected (RR=1.75; p=0.07) which disappears after controlling for individual-level characteristics.
Conclusions: A geographically targeted CPR training strategy which is tailored to individual and neighborhood population characteristics may be effective in reducing existing disparities in the provision of bystander CPR for out-of-hospital cardiac arrest.
Copyright © 2013 Elsevier Ireland Ltd. All rights reserved.
Conflict of interest statement
There are no conflicts of interest.
Figures
Comment in
-
Bystander CPR: location, location, location.Resuscitation. 2013 Jun;84(6):711-2. doi: 10.1016/j.resuscitation.2013.03.008. Epub 2013 Mar 13. Resuscitation. 2013. PMID: 23499853 No abstract available.
References
-
- Ong ME, Chiam TF, Ng FS, et al. Reducing ambulance response times using geospatial-time analysis of ambulance deployment. Acad Emerg Med. 2010;17:951–7. - PubMed
-
- Ott WE. GIS in EMS. JEMS. 2003;28:89–91. - PubMed
-
- Peleg K, Pliskin JS. A geographic information system simulation model of EMS: reducing ambulance response time. Am J Emerg Med. 2004;22:164–70. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
