

Sarcoidosis presenting with massive pleural effusion and elevated serum and pleural fluid carbohydrate antigen-125 levels
- PMID: 23319994
- PMCID: PMC3538185
- DOI: 10.4046/trd.2012.73.6.320
Sarcoidosis presenting with massive pleural effusion and elevated serum and pleural fluid carbohydrate antigen-125 levels
Abstract
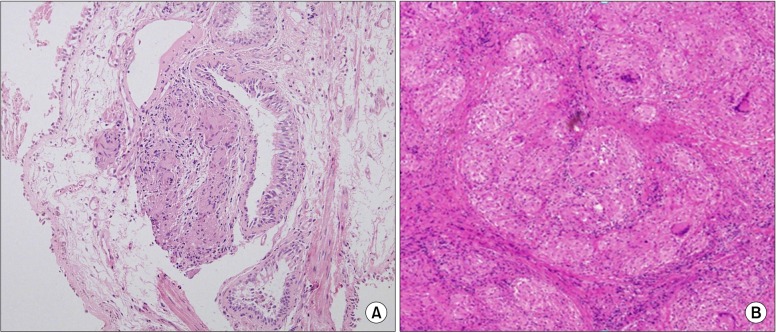
A 55-year-old woman was admitted for an elevated serum carbohydrate antigen-125 (CA-125) level, and a left pleural effusion, which were detected at a routine health examination. Computed tomography of the chest was performed upon admission, revealing extensive bilateral paratracheal and mediastinal lymph node enlargement with a massive left-sided pleural effusion. Subsequent analysis of the pleural fluid demonstrated consistency with an exudate, no evidence of malignant cells, and a normal adenosine deaminase. However, the pleural fluid and serum CA-125 levels were 2,846.8 U/mL and 229.5 U/mL, respectively. A positron emission tomography did not reveal any primary focus of malignancy. Finally, a surgical mediastinoscopic biopsy of several mediastinal lymph nodes was performed, revealing non-necrotizing granulomas, consistent with sarcoidosis. After a month of treatment of prednisolone, the left pleural effusion had resolved, and after 2 months the serum CA-125 level was normalized.
Keywords: CA-125 Antigen; Pleural Effusion; Sarcoidosis.
Figures


Similar articles
-
Massive pericardial effusion causing cardiac tamponade accompanied by elevated CA-125 and thoracic lymphadenopathy in sarcoidosis: a case report.Int J Surg Case Rep. 2020;72:355-360. doi: 10.1016/j.ijscr.2020.06.037. Epub 2020 Jun 13. Int J Surg Case Rep. 2020. PMID: 32563820 Free PMC article.
-
Rapidly recurring massive pleural effusion as the initial presentation of sarcoidosis: A case report.Medicine (Baltimore). 2021 Feb 12;100(6):e24027. doi: 10.1097/MD.0000000000024027. Medicine (Baltimore). 2021. PMID: 33578518 Free PMC article.
-
Pleural sarcoidosis diagnosed on the basis of an increased CD4/CD8 lymphocyte ratio in pleural effusion fluid: a case report.J Med Case Rep. 2015 Aug 14;9:170. doi: 10.1186/s13256-015-0656-y. J Med Case Rep. 2015. PMID: 26271927 Free PMC article.
-
[Idiopathic plasmacytic lymphadenopathy with polyclonal hyperimmunoglobulinemia and pleural effusion].Nihon Kokyuki Gakkai Zasshi. 2000 Apr;38(4):288-92. Nihon Kokyuki Gakkai Zasshi. 2000. PMID: 10879032 Review. Japanese.
-
Left Lung Neoplasms and Bilateral Pleural Effusion Combined Elevated Carcinoembryonic Antigen in Pleural Effusion with Negative Result of Thoracoscopy Pleural Biopsy Misdiagnosed as Lung Carcinoma Ultimately Confirmed Pulmonary Sarcomatoid Carcinoma by CT-guided Percutaneous Lung Biopsy: a Case Report and Literature Review.Clin Lab. 2019 Aug 1;65(8). doi: 10.7754/Clin.Lab.2019.190127. Clin Lab. 2019. PMID: 31414757 Review.
Cited by
-
Diagnostic value of elevated serum carbohydrate antigen 125 level in sarcoidosis.World J Clin Cases. 2022 Aug 16;10(23):8141-8151. doi: 10.12998/wjcc.v10.i23.8141. World J Clin Cases. 2022. PMID: 36159536 Free PMC article.
-
Pleural Sarcoidosis and Occult Lymphatic Anthracosis: An Unusual Symptomatic Association.Eur J Case Rep Intern Med. 2020 Mar 17;7(5):001479. doi: 10.12890/2020_001479. eCollection 2020. Eur J Case Rep Intern Med. 2020. PMID: 32399439 Free PMC article.
-
Multisystemic Sarcoidosis Presenting With Leg Ulcers, Pancytopenia, and Polyserositis Was Successfully Treated With Glucocorticoids: A Case Report and Literature Review.Front Med (Lausanne). 2022 Feb 15;8:803852. doi: 10.3389/fmed.2021.803852. eCollection 2021. Front Med (Lausanne). 2022. PMID: 35242768 Free PMC article.
-
Sarcoidosis associated massive pleural Effusion: Case report and literature review.Respir Med Case Rep. 2025 Jul 3;57:102247. doi: 10.1016/j.rmcr.2025.102247. eCollection 2025. Respir Med Case Rep. 2025. PMID: 40799675 Free PMC article.
-
Massive pericardial effusion causing cardiac tamponade accompanied by elevated CA-125 and thoracic lymphadenopathy in sarcoidosis: a case report.Int J Surg Case Rep. 2020;72:355-360. doi: 10.1016/j.ijscr.2020.06.037. Epub 2020 Jun 13. Int J Surg Case Rep. 2020. PMID: 32563820 Free PMC article.
References
-
- Huggins JT, Doelken P, Sahn SA, King L, Judson MA. Pleural effusions in a series of 181 outpatients with sarcoidosis. Chest. 2006;129:1599–1604. - PubMed
-
- Kalluri M, Judson MA. Sarcoidosis associated with an elevated serum CA 125 level: description of a case and a review of the literature. Am J Med Sci. 2007;334:441–443. - PubMed
-
- Salerno D. Sarcoidosis pleural effusion: a not so common feature of a well known pulmonary disease. Respir Care. 2010;55:478–480. - PubMed
-
- Soskel NT, Sharma OP. Pleural involvement in sarcoidosis. Curr Opin Pulm Med. 2000;6:455–468. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
