

Traditional transcutaneous approaches in head and neck surgery
- PMID: 23320058
- PMCID: PMC3544212
- DOI: 10.3205/cto000088
Traditional transcutaneous approaches in head and neck surgery
Abstract
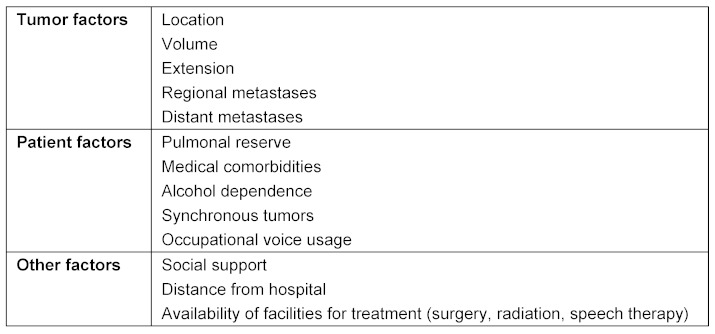
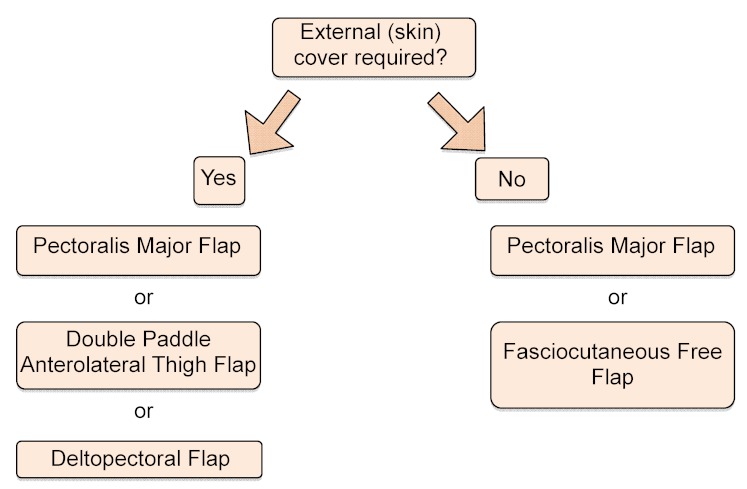
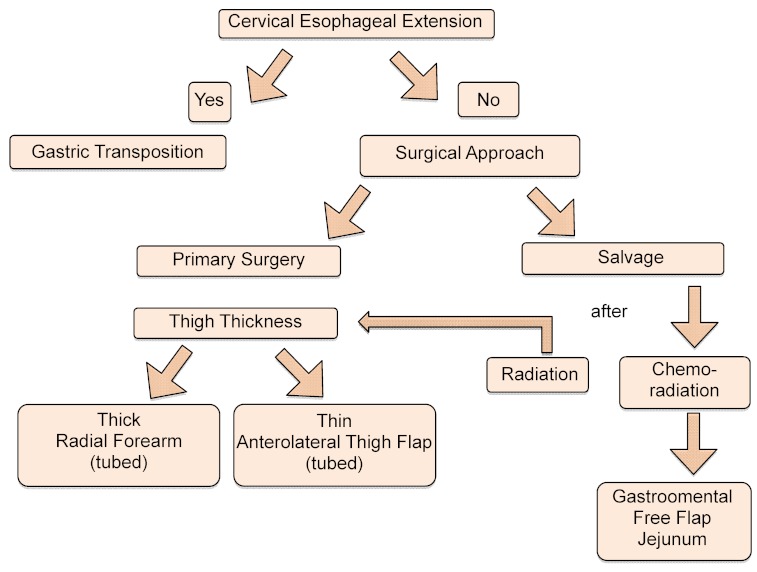
The treatment of laryngeal and hypopharyngeal malignancies remains a challenging task for the head and neck surgeon as the chosen treatment modality often has to bridge the gap between oncologically sound radicality and preservation of function. Due to the increase in transoral laser surgery in early tumor stages and chemoradiation in advanced stages, the usage of traditional transcutaneous approaches has decreased over the recent past. In addition, the need for a function-sparing surgical approach as well as highest possible quality of life has become evident. In view of these facts, rationale and importance of traditional transcutaneous approaches to the treatment of laryngeal and hypopharyngeal malignancies are discussed in a contemporary background. The transcutaneous open partial laryngectomies remain a valuable tool in the surgeon's armamentarium for the treatment of early and advanced laryngeal carcinomas, especially in cases of impossible laryngeal overview using the rigid laryngoscope. Open partial laryngetomies offer superior overview and oncologic safety at the anterior commissure, especially in recurrencies. In select advanced cases and salvage settings, the supracricoid laryngectomy offers a valuable tool for function-preserving but oncologically safe surgical therapy at the cost of high postoperative morbidity and a very demanding rehabilitation of swallowing.In hypopharyngeal malignancies, the increasing use of transoral laser surgery has led to a decline in transcutaneous resections via partial pharyngectomy with partial laryngectomy in early tumor stages. In advanced stages of tumors of the piriform sinus and the postcricoid area with involvement of the larynx, total laryngectomy with partial pharyngectomy is an oncologically safe approach. The radical surgical approach using circumferent laryngopharyngectomy with/without esophagectomy is indicated in salvage cases with advanced recurrences or as a primary surgical approach in patients where chemoradiation does not offer sufficient oncologic control or preservation of function. In cases with impending reconstruction, fasciocutaneous free flaps (anterolateral thigh flap, radial forearm flap) seem to offer superior results to enteric flaps in cases where the cervical esophagus is not involved leading to better voice rehabilitation with fewer complications and postoperative morbidity. In salvage situations, the Gastroomental Free Flap has proven to be a valuable tool.In conclusion, the choice of a surgical treatment modality is influenced by the patient's anatomy, tumor size and location as well as the surgeon's personal expertise.
Figures

Similar articles
-
[Traditional transcutaneous approaches in head & neck surgery].Laryngorhinootologie. 2012 Mar;91 Suppl 1:S63-85. doi: 10.1055/s-0031-1297242. Epub 2012 Mar 28. Laryngorhinootologie. 2012. PMID: 22456920 Review. German.
-
[Functional long-term results following hemipharyngo-hemilaryngectomy and microvascular reconstruction using the radial forearm flap].Laryngorhinootologie. 2002 Mar;81(3):233-42. doi: 10.1055/s-2002-25036. Laryngorhinootologie. 2002. PMID: 11967777 German.
-
Current trends in initial management of laryngeal cancer: the declining use of open surgery.Eur Arch Otorhinolaryngol. 2009 Sep;266(9):1333-52. doi: 10.1007/s00405-009-1028-2. Epub 2009 Jul 14. Eur Arch Otorhinolaryngol. 2009. PMID: 19597837 Review.
-
Treatment outcome in patients undergoing surgery for carcinoma larynx and hypopharynx: a follow-up study.Acta Otolaryngol. 2009 Dec;129(12):1480-5. doi: 10.3109/00016480902748520. Acta Otolaryngol. 2009. PMID: 19922101
-
Voice and swallowing outcomes of an organ-preservation trial for advanced laryngeal cancer.Int J Radiat Oncol Biol Phys. 2005 Dec 1;63(5):1395-9. doi: 10.1016/j.ijrobp.2005.05.004. Epub 2005 Aug 8. Int J Radiat Oncol Biol Phys. 2005. PMID: 16087298 Clinical Trial.
Cited by
-
Effect of voice training in the voice rehabilitation of patients with vocal cord polyps after surgery.Exp Ther Med. 2014 Apr;7(4):877-880. doi: 10.3892/etm.2014.1499. Epub 2014 Jan 23. Exp Ther Med. 2014. PMID: 24669244 Free PMC article.
References
-
- Ambrosch P, Rödel R, Kron M, Steiner W. Die transorale Lasermikrochirurgie des Larynxkarzinoms. Der Onkologe. 2001;7:505–512. doi: 10.1007/s007610170103. Available from: http://dx.doi.org/10.1007/s007610170103. - DOI - DOI
-
- Induction chemotherapy plus radiation compared with surgery plus radiation in patients with advanced laryngeal cancer. The Department of Veterans Affairs Laryngeal Cancer Study Group. N Engl J Med. 1991 Jun;324(24):1685–1690. doi: 10.1056/NEJM199106133242402. Available from: http://dx.doi.org/10.1056/NEJM199106133242402. - DOI - DOI - PubMed
-
- Forastiere AA, Goepfert H, Maor M, Pajak TF, Weber R, Morrison W, Glisson B, Trotti A, Ridge JA, Chao C, Peters G, Lee DJ, Leaf A, Ensley J, Cooper J. Concurrent chemotherapy and radiotherapy for organ preservation in advanced laryngeal cancer. N Engl J Med. 2003 Nov;349(22):2091–2098. doi: 10.1056/NEJMoa031317. Available from: http://dx.doi.org/10.1056/NEJMoa031317. - DOI - DOI - PubMed
-
- Davies L, Welch HG. Epidemiology of head and neck cancer in the United States. Otolaryngol Head Neck Surg. 2006 Sep;135(3):451–457. doi: 10.1016/j.otohns.2006.01.029. Available from: http://dx.doi.org/10.1016/j.otohns.2006.01.029. - DOI - DOI - PubMed
-
- Jemal A, Siegel R, Ward E, Murray T, Xu J, Thun MJ. Cancer statistics, 2007. CA Cancer J Clin. 2007 Jan-Feb;57(1):43–66. doi: 10.3322/canjclin.57.1.43. Available from: http://dx.doi.org/10.3322/canjclin.57.1.43. - DOI - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
