

Environmental factors associated with disease progression after the first demyelinating event: results from the multi-center SET study
- PMID: 23320113
- PMCID: PMC3540021
- DOI: 10.1371/journal.pone.0053996
Environmental factors associated with disease progression after the first demyelinating event: results from the multi-center SET study
Abstract
Objectives: To investigate the associations of environmental MS risk factors with clinical and MRI measures of progression in high-risk clinically isolated syndromes (CIS) after the first demyelinating event.
Methods: We analyzed 211 CIS patients (age: 28.9±7.8 years) enrolled in the SET study, a multi-center study of high-risk CIS patients. Pre-treatment samples were analyzed for IgG antibodies against cytomegalovirus (anti-CMV), Epstein Barr virus (EBV) early nuclear antigen-1 (EBNA-1), viral capsid antigen (VCA), early antigen-diffuse (EA-D), 25 hydroxy-vitamin D3 and cotinine levels and HLA DRB1*1501 status. The inclusion criteria required evaluation within 4 months of the initial demyelinating event, 2 or more brain MRI lesions and the presence of two or more oligoclonal bands in cerebrospinal fluid. All patients were treated with interferon-beta. Clinical and MRI assessments were obtained at baseline, 6, 12, and 24 months.
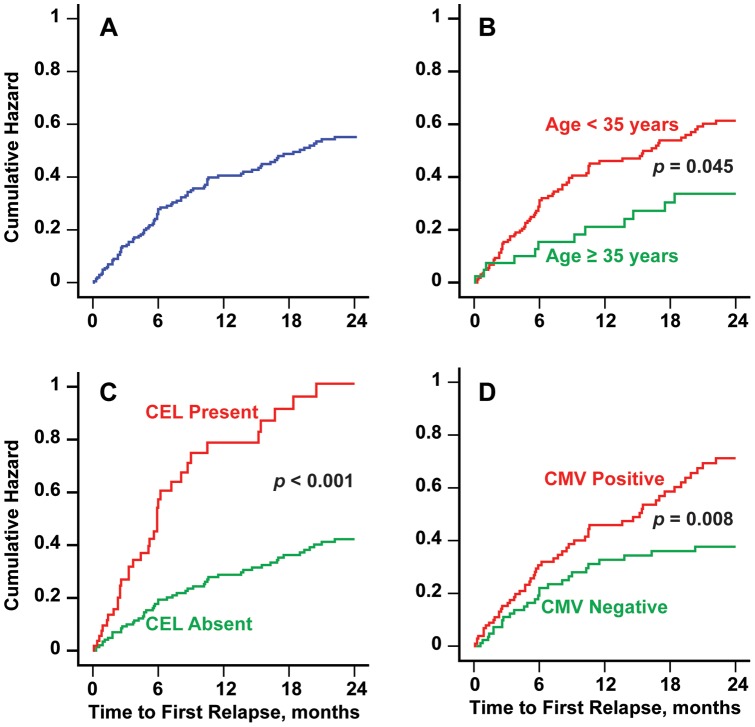
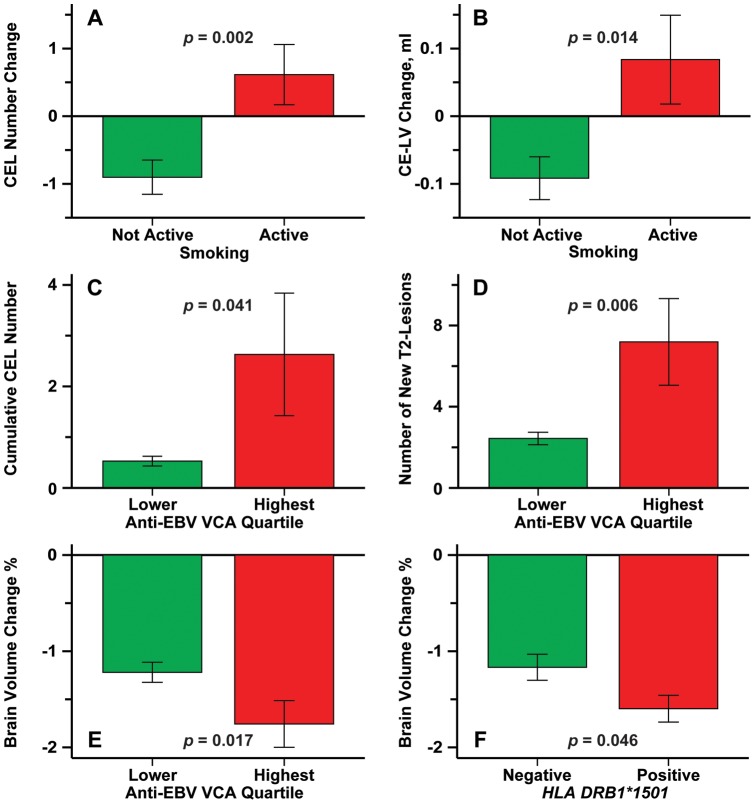
Results: The time to first relapse decreased and the number of relapses increased with anti-CMV IgG positivity. Smoking was associated with increased number and volume of contrast-enhancing lesions (CEL) during the 2-year period. The cumulative number of CEL and T2 lesions during the 2-year period was greater for individuals in the highest quartile of anti-EBV VCA IgG antibodies. The percent loss of brain volume was increased for those in the highest quartile of with anti-EBV VCA IgG antibodies.
Conclusions: Relapses in CIS patients were associated with CMV positivity whereas anti-EBV VCA positivity was associated with progression on MRI measures, including accumulation of CEL and T2 lesions and development of brain atrophy.
Conflict of interest statement
Figures
References
-
- Ascherio A, Munger KL (2007) Environmental risk factors for multiple sclerosis. Part II: Noninfectious factors. Ann Neurol 61: 504–513. - PubMed
-
- Ascherio A, Munger KL (2007) Environmental risk factors for multiple sclerosis. Part I: the role of infection. Ann Neurol 61: 288–299. - PubMed
-
- Zivadinov R, Weinstock-Guttman B, Zorzon M, Uxa L, Serafin M, et al. (2009) Gene-environment interactions between HLA B7/A2, EBV antibodies are associated with MRI injury in multiple sclerosis. J Neuroimmunol 209: 123–130. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
