

Developing a mobility protocol for early mobilization of patients in a surgical/trauma ICU
- PMID: 23320154
- PMCID: PMC3539434
- DOI: 10.1155/2012/964547
Developing a mobility protocol for early mobilization of patients in a surgical/trauma ICU
Abstract
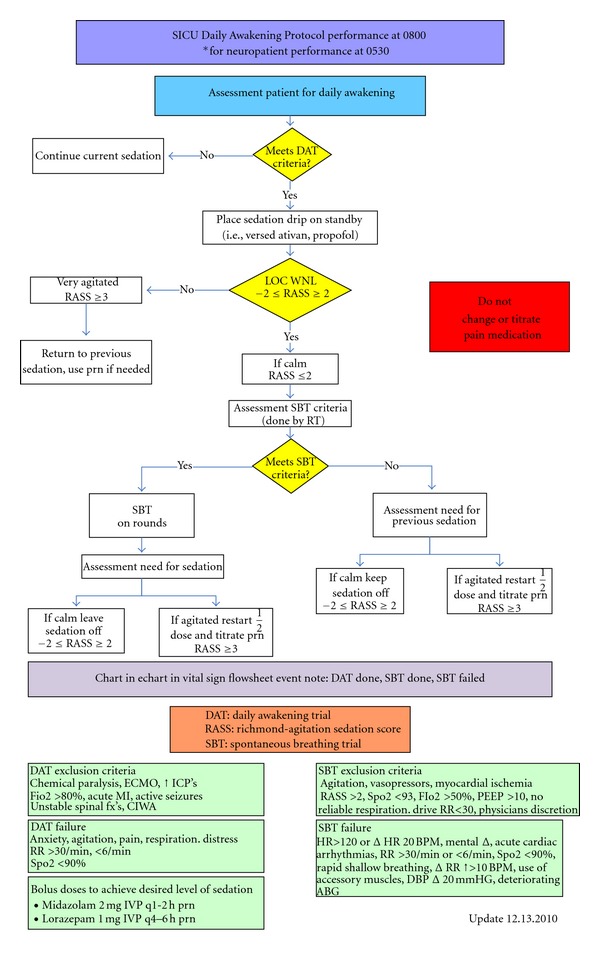
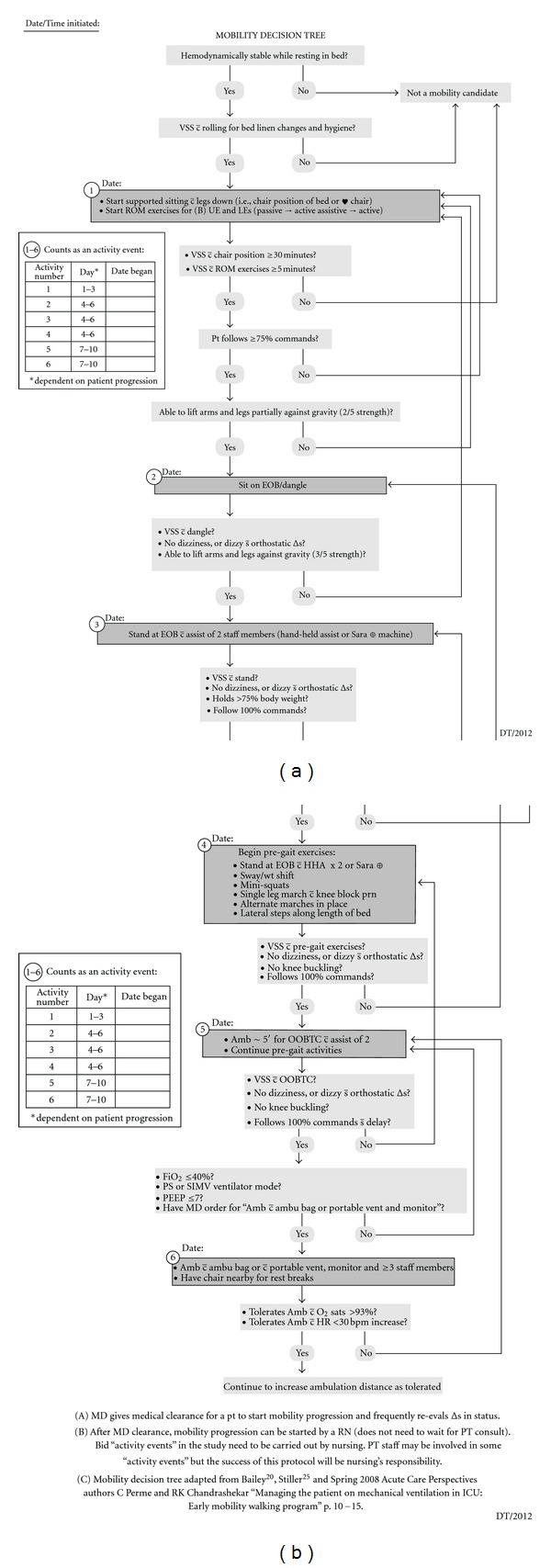
As technology and medications have improved and increased, survival rates are also increasing in intensive care units (ICUs), so it is now important to focus on improving the patient outcomes and recovery. To do this, ICU patients need to be assessed and started on an early mobility program, if stable. While the early mobilization of the ICU patients is not without risk, the current literature has demonstrated that patients can be safely and feasibly mobilized, even while requiring mechanical ventilation. These patients are at a high risk for muscle deconditioning due to limited mobility from numerous monitoring equipment and multiple medical conditions. Frequently, a critically ill patient only receives movement from nurses; such as, being turned side to side, pulled up in bed, or transferred from bed to a stretcher for a test. The implementation of an early mobility protocol that can be used by critical care nurses is important for positive patient outcomes minimizing the functional decline due to an ICU stay. This paper describes a pilot study to evaluate an early mobilization protocol to test the safety and feasibility for mechanically ventilated patients in a surgical trauma ICU in conjunction with the current unit standards.
Figures
Similar articles
-
PROtocol-based MObilizaTION on intensive care units: stepped-wedge, cluster-randomized pilot study (Pro-Motion).Nurs Crit Care. 2020 Nov;25(6):368-375. doi: 10.1111/nicc.12438. Epub 2019 May 24. Nurs Crit Care. 2020. PMID: 31125163 Clinical Trial.
-
Mobilization practices in the ICU: A nationwide 1-day point- prevalence study in Brazil.PLoS One. 2020 Apr 2;15(4):e0230971. doi: 10.1371/journal.pone.0230971. eCollection 2020. PLoS One. 2020. PMID: 32240249 Free PMC article.
-
Early Rehabilitation in the Medical and Surgical Intensive Care Units for Patients With and Without Mechanical Ventilation: An Interprofessional Performance Improvement Project.PM R. 2017 Feb;9(2):113-119. doi: 10.1016/j.pmrj.2016.06.015. Epub 2016 Jun 23. PM R. 2017. PMID: 27346093
-
Early Mobilization and Rehabilitation in the ICU: Moving Back to the Future.Respir Care. 2016 Jul;61(7):971-9. doi: 10.4187/respcare.04741. Epub 2016 Apr 19. Respir Care. 2016. PMID: 27094396 Review.
-
The effect of early mobilization in critically ill patients: A meta-analysis.Nurs Crit Care. 2020 Nov;25(6):360-367. doi: 10.1111/nicc.12455. Epub 2019 Jun 20. Nurs Crit Care. 2020. PMID: 31219229
Cited by
-
Assessing the impact of early progressive mobilization on moderate-to-severe traumatic brain injury: a randomized controlled trial.Crit Care. 2024 May 22;28(1):172. doi: 10.1186/s13054-024-04940-0. Crit Care. 2024. PMID: 38778416 Free PMC article. Clinical Trial.
-
Role of ambulation to prevent venous thromboembolism in medical patients: where do we stand?J Vasc Bras. 2019 Jun 25;18:e20180107. doi: 10.1590/1677-5449.180107. J Vasc Bras. 2019. PMID: 31360151 Free PMC article. Review.
-
Association between early ambulation exercise and short-term postoperative recovery after open transforaminal lumbar interbody fusion: a single center retrospective analysis.BMC Musculoskelet Disord. 2023 May 4;24(1):345. doi: 10.1186/s12891-023-06395-w. BMC Musculoskelet Disord. 2023. PMID: 37143006 Free PMC article.
-
Association of early mobility with the incidence of deep-vein thrombosis and mortality among critically ill patients: a post hoc analysis of PREVENT trial.Crit Care. 2023 Mar 3;27(1):83. doi: 10.1186/s13054-023-04333-9. Crit Care. 2023. PMID: 36869382 Free PMC article.
-
Clinicians' knowledge and attitude towards early mobilization in intensive care units in Ethiopian tertiary hospitals: A multi-centre study.SAGE Open Med. 2023 May 15;11:20503121231172348. doi: 10.1177/20503121231172348. eCollection 2023. SAGE Open Med. 2023. PMID: 37205156 Free PMC article.
References
-
- Combes A, Costa MA, Trouillet JL, et al. Morbidity, mortality, and quality-of-life outcomes of patients requiring ≥14 days of mechanical ventilation. Critical Care Medicine. 2003;31(5):1373–1381. - PubMed
-
- Herridge MS, Cheung AM, Tansey CM, et al. One-year outcomes in survivors of the acute respiratory distress syndrome. New England Journal of Medicine. 2003;348(8):683–693. - PubMed
-
- Needham DM. Mobilizing patients in the intensive care unit: improving neuromuscular weakness and physical function. Journal of the American Medical Association. 2008;300(14):1685–1690. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
