

Fast-track surgery in gynaecology and gynaecologic oncology: a review of a rolling clinical audit
- PMID: 23320193
- PMCID: PMC3540771
- DOI: 10.5402/2012/368014
Fast-track surgery in gynaecology and gynaecologic oncology: a review of a rolling clinical audit
Abstract
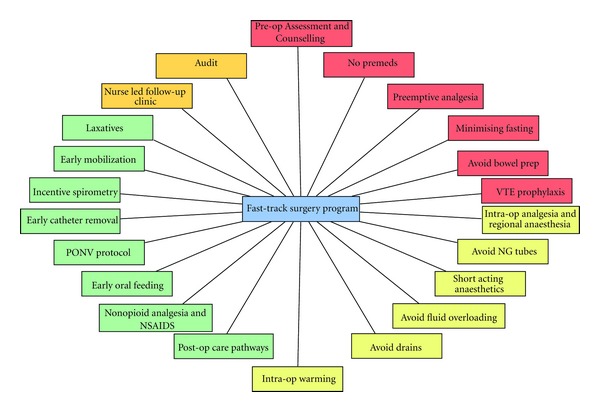
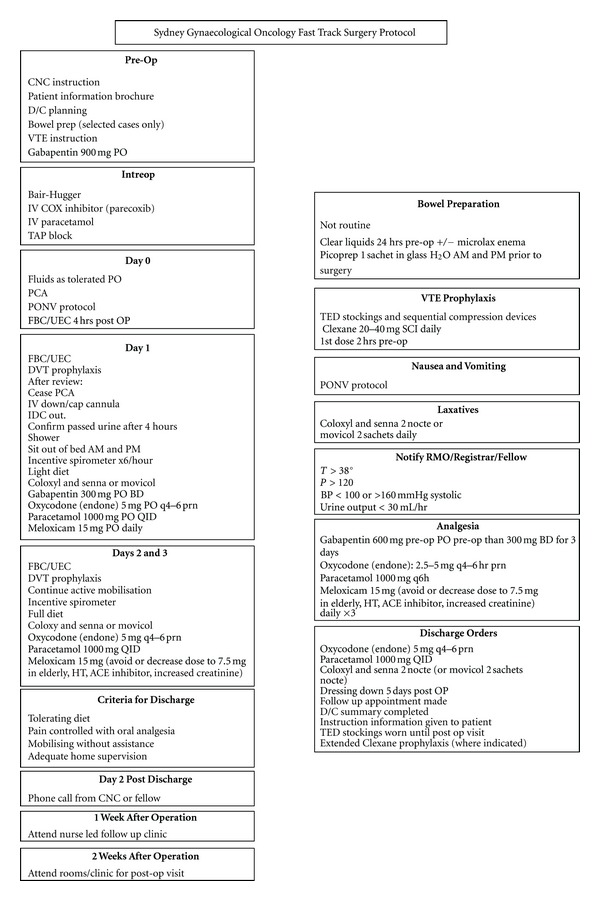
Clinical audit is the process by which clinicians are able to demonstrate to themselves, their patients, hospital administrators, and healthcare financial providers the outcome and safety of their clinical practice. It is a process by which the public can be assured of safety and outcomes. A fast-track surgery program was initiated in January 2008, and this paper represents a rolling clinical audit of the outcomes of that program until the end of June 2012. Three hundred and eighty-nine patients underwent fast track surgical management after having a laparotomy for suspected or confirmed gynaecological cancer. There were no exclusions and the data presented represents the practice and outcomes of all patients referred to a single gynaecological oncologist. The majority of patients were deemed to have complex surgical procedures performed usually through a vertical midline incision. One third of patients had a nonzero performance status, median weight was 68 kilograms, and median BMI was 26.5 with 31% being classified as obese. Median operating time was 2.25 hours, and the median estimated blood loss was 175 mL. Overall the median length of stay (LOS) was 3 days with 95% of patients tolerating early oral feeding. Four percent of patients required readmission, and 0.5% were required to return to the operating room. Whilst the wound infection rate was 2.6%, there were no ureteric, bowel or neurovascular injuries. Overall there were 2 bladder injuries (0.5%), and the incidence of venous thromboembolism was 1%. Subset analysis was also undertaken. Whilst a number of variables were associated with reduced LOS, on multivariate analysis, benign pathology, shorter operating time, and the ability to tolerate early oral feeding were found to be significant. The data and experience presented is the largest and most extensive reported in the literature relating to fast-track surgery in gynaecology and gynaecologic oncology. The public can be reassured of the safety and improved outcomes that can be achieved after the introduction of such a program.
Figures
References
-
- RACS. A Guide By the Royal Australian College of Surgeons. Surgical Audit and Peer Review. Melbourne, Australia: Royal Australian College of Surgeons; 2008.
-
- Kehlet H. Fast-track colorectal surgery. The Lancet. 2008;371(9615):791–793. - PubMed
-
- Kehlet H, Wilmore DW. Multimodal strategies to improve surgical outcome. American Journal of Surgery. 2002;183(6):630–641. - PubMed
LinkOut - more resources
Full Text Sources
Medical